

Artificial sweeteners and risk of incident cardiovascular disease and mortality: evidence from UK Biobank
- PMID: 38965574
- PMCID: PMC11225337
- DOI: 10.1186/s12933-024-02333-9
Artificial sweeteners and risk of incident cardiovascular disease and mortality: evidence from UK Biobank
Abstract
Background: Artificial sweeteners are widely popular worldwide as substitutes for sugar or caloric sweeteners, but there are still several important unknowns and controversies regarding their associations with cardiovascular disease (CVD). We aimed to extensively assess the association and subgroup variability between artificial sweeteners and CVD and CVD mortality in the UK Biobank cohort, and further investigate the modification effects of genetic susceptibility and the mediation role of type 2 diabetes mellitus (T2DM).
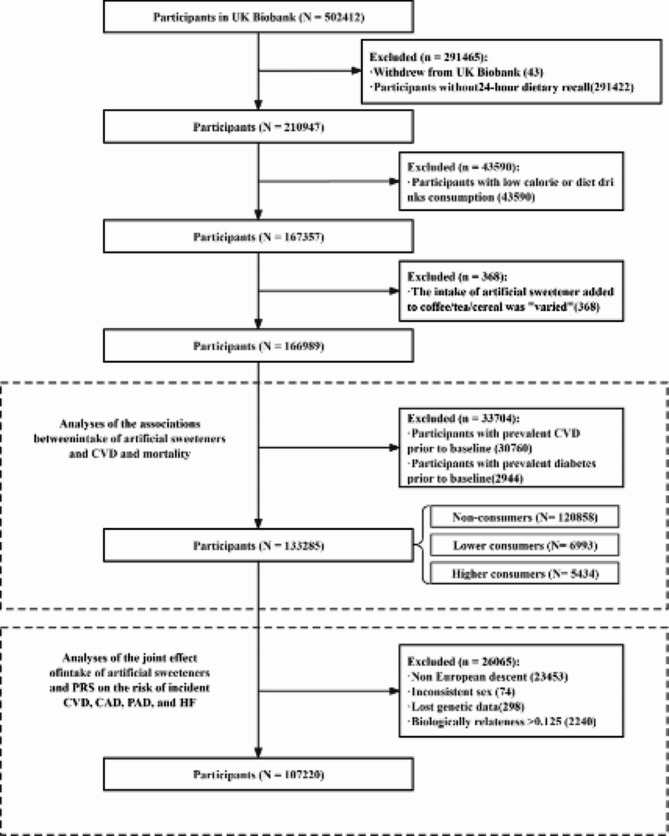
Methods: This study included 133,285 participants in the UK Biobank who were free of CVD and diabetes at recruitment. Artificial sweetener intake was obtained from repeated 24-hour diet recalls. Cox proportional hazard models were used to estimate HRs. Genetic predisposition was estimated using the polygenic risk score (PRS). Furthermore, time-dependent mediation was performed.
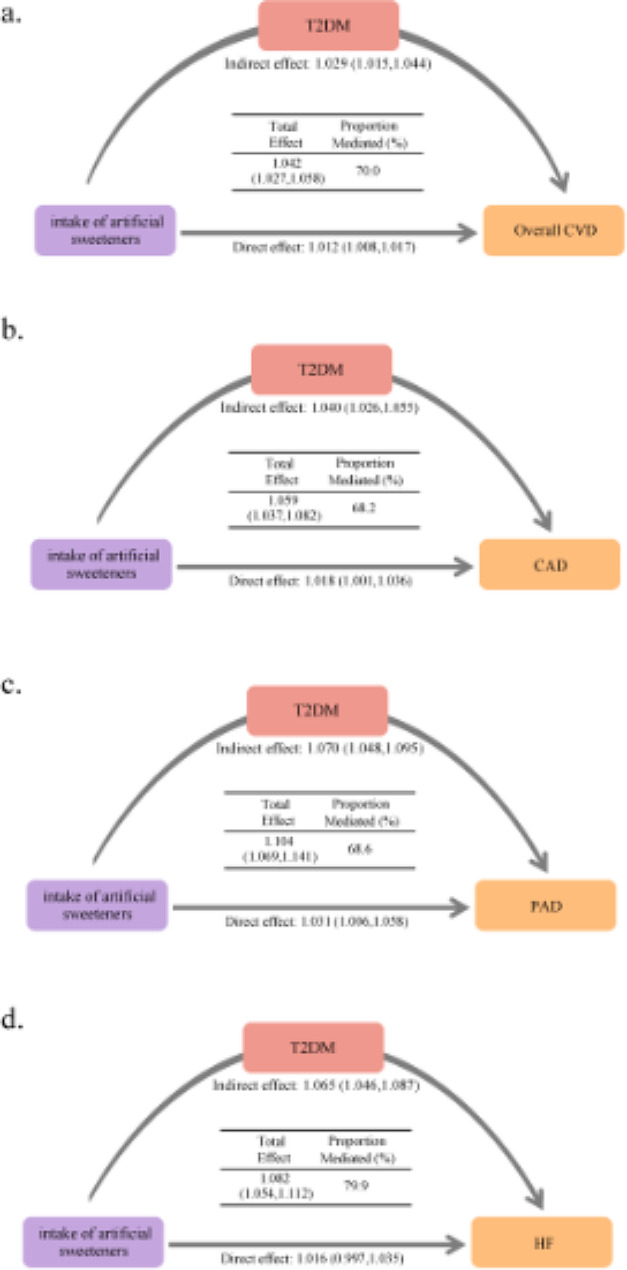
Results: In our study, artificial sweetener intake (each teaspoon increase) was significantly associated with an increased risk of incident overall CVD (HR1.012, 95%CI: 1.008,1.017), coronary artery disease (CAD) (HR: 1.018, 95%CI: 1.001,1.035), peripheral arterial disease (PAD) (HR: 1.035, 95%CI: 1.010,1.061), and marginally significantly associated with heart failure (HF) risk (HR: 1.018, 95%CI: 0.999,1.038). In stratified analyses, non-whites were at greater risk of incident overall CVD from artificial sweetener. People with no obesity (BMI < 30 kg/m2) also tended to be at greater risk of incident CVD from artificial sweetener, although the obesity interaction is not significant. Meanwhile, the CVD risk associated with artificial sweeteners is independent of genetic susceptibility, and no significant interaction exists between genetic susceptibility and artificial sweeteners in terms of either additive or multiplicative effects. Furthermore, our study revealed that the relationship between artificial sweetener intake and overall CVD is significantly mediated, in large part, by prior T2DM (proportion of indirect effect: 70.0%). In specific CVD subtypes (CAD, PAD, and HF), the proportion of indirect effects ranges from 68.2 to 79.9%.
Conclusions: Our findings suggest significant or marginally significant associations between artificial sweeteners and CVD and its subtypes (CAD, PAD, and HF). The associations are independent of genetic predisposition and are mediated primarily by T2DM. Therefore, the large-scale application of artificial sweeteners should be prudent, and the responses of individuals with different characteristics to artificial sweeteners should be better characterized to guide consumers' artificial sweeteners consumption behavior.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
