

Associations of metabolic changes and polygenic risk scores with cardiovascular outcomes and all-cause mortality across BMI categories: a prospective cohort study
- PMID: 38965592
- PMCID: PMC11225301
- DOI: 10.1186/s12933-024-02332-w
Associations of metabolic changes and polygenic risk scores with cardiovascular outcomes and all-cause mortality across BMI categories: a prospective cohort study
Abstract
Background: Associations between metabolic status and metabolic changes with the risk of cardiovascular outcomes have been reported. However, the role of genetic susceptibility underlying these associations remains unexplored. We aimed to examine how metabolic status, metabolic transitions, and genetic susceptibility collectively impact cardiovascular outcomes and all-cause mortality across diverse body mass index (BMI) categories.
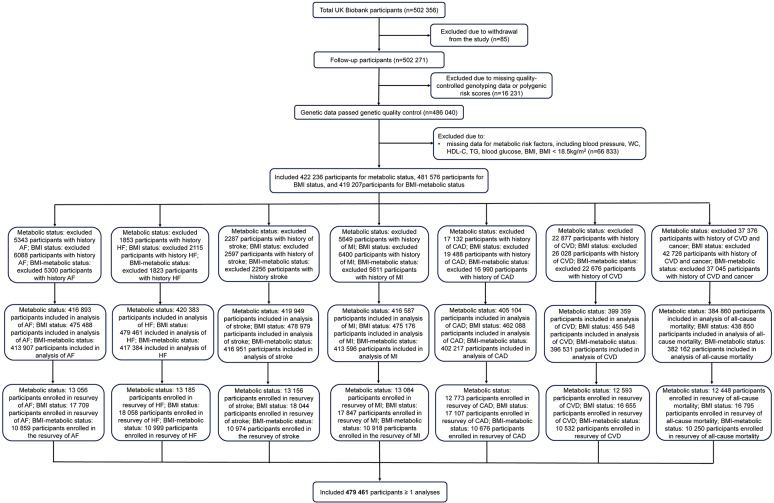
Methods: In our analysis of the UK Biobank, we included a total of 481,576 participants (mean age: 56.55; male: 45.9%) at baseline. Metabolically healthy (MH) status was defined by the presence of < 3 abnormal components (waist circumstance, blood pressure, blood glucose, triglycerides, and high-density lipoprotein cholesterol). Normal weight, overweight, and obesity were defined as 18.5 ≤ BMI < 25 kg/m2, 25 ≤ BMI < 30 kg/m2, and BMI ≥ 30 kg/m2, respectively. Genetic predisposition was estimated using the polygenic risk score (PRS). Cox regressions were performed to evaluate the associations of metabolic status, metabolic transitions, and PRS with cardiovascular outcomes and all-cause mortality across BMI categories.
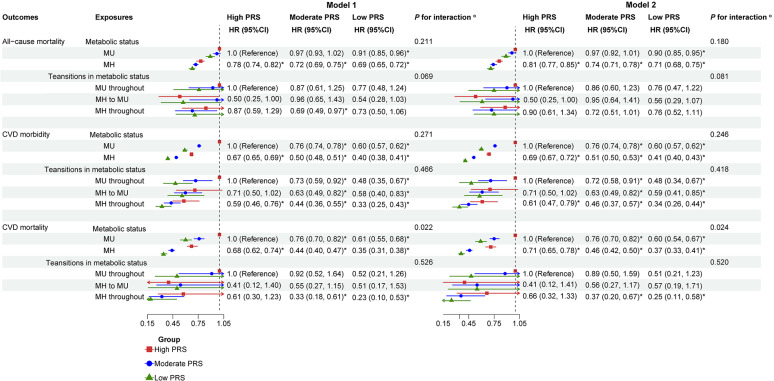
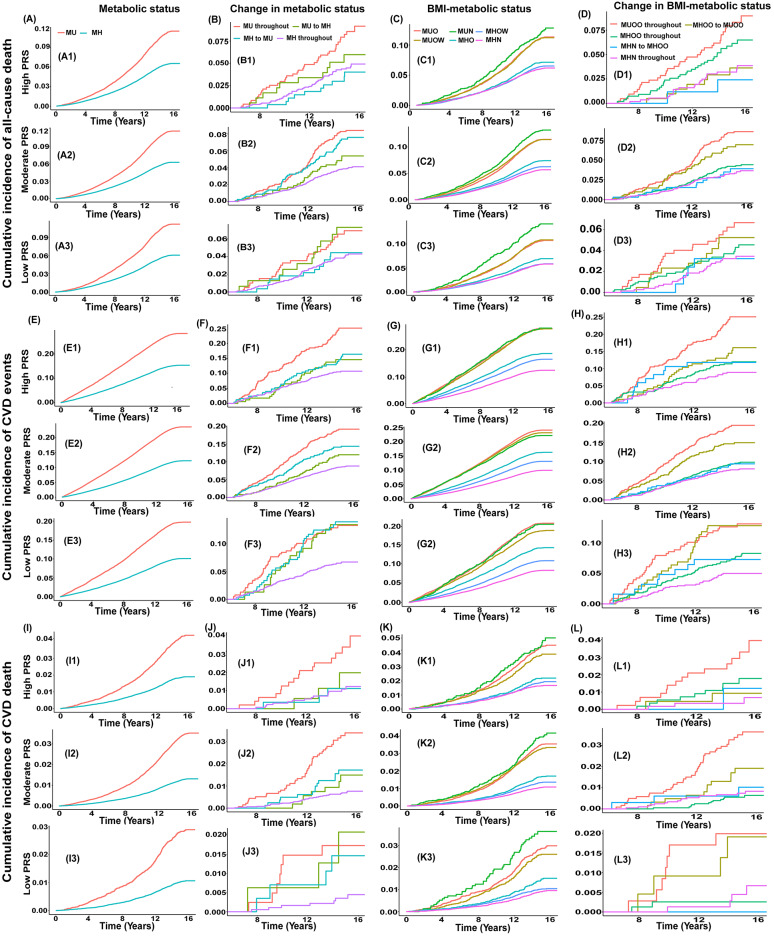
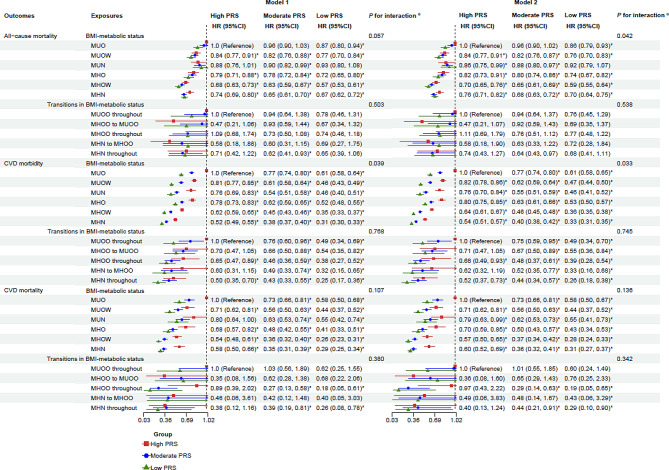
Results: During a median follow-up of 14.38 years, 31,883 (7.3%) all-cause deaths, 8133 (1.8%) cardiovascular disease (CVD) deaths, and 67,260 (14.8%) CVD cases were documented. Among those with a high PRS, individuals classified as metabolically healthy overweight had the lowest risk of all-cause mortality (hazard ratios [HR] 0.70; 95% confidence interval [CI] 0.65, 0.76) and CVD mortality (HR 0.57; 95% CI 0.50, 0.64) compared to those who were metabolically unhealthy obesity, with the beneficial associations appearing to be greater in the moderate and low PRS groups. Individuals who were metabolically healthy normal weight had the lowest risk of CVD morbidity (HR 0.54; 95% CI 0.51, 0.57). Furthermore, the inverse associations of metabolic status and PRS with cardiovascular outcomes and all-cause mortality across BMI categories were more pronounced among individuals younger than 65 years (Pinteraction < 0.05). Additionally, the combined protective effects of metabolic transitions and PRS on these outcomes among BMI categories were observed.
Conclusions: MH status and a low PRS are associated with a lower risk of adverse cardiovascular outcomes and all-cause mortality across all BMI categories. This protective effect is particularly pronounced in individuals younger than 65 years. Further research is required to confirm these findings in diverse populations and to investigate the underlying mechanisms involved.
Keywords: All-cause mortality; Cardiovascular disease; Metabolic change; Metabolic health; Metabolic syndrome; Polygenic risk scores.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Metabolically healthy obesity, transition to unhealthy metabolic status, and vascular disease in Chinese adults: A cohort study.PLoS Med. 2020 Oct 30;17(10):e1003351. doi: 10.1371/journal.pmed.1003351. eCollection 2020 Oct. PLoS Med. 2020. PMID: 33125374 Free PMC article.
-
Transition from metabolic healthy to unhealthy phenotypes and association with cardiovascular disease risk across BMI categories in 90 257 women (the Nurses' Health Study): 30 year follow-up from a prospective cohort study.Lancet Diabetes Endocrinol. 2018 Sep;6(9):714-724. doi: 10.1016/S2213-8587(18)30137-2. Epub 2018 May 31. Lancet Diabetes Endocrinol. 2018. PMID: 29859908
-
Joint and interactive associations of body mass index and genetic factors with cardiovascular disease: a prospective study in UK Biobank.BMC Public Health. 2024 Sep 2;24(1):2371. doi: 10.1186/s12889-024-19916-6. BMC Public Health. 2024. PMID: 39223569 Free PMC article.
-
Metabolically healthy overweight/obesity are associated with increased risk of cardiovascular disease in adults, even in the absence of metabolic risk factors: A systematic review and meta-analysis of prospective cohort studies.Obes Rev. 2020 Dec;21(12):e13127. doi: 10.1111/obr.13127. Epub 2020 Sep 1. Obes Rev. 2020. PMID: 32869512
-
Polygenic Risk Score Implementation into Clinical Practice for Primary Prevention of Cardiometabolic Disease.Genes (Basel). 2024 Dec 9;15(12):1581. doi: 10.3390/genes15121581. Genes (Basel). 2024. PMID: 39766848 Free PMC article. Review.
Cited by
-
Remnant cholesterol inflammatory index and its association with all-cause and cause-specific mortality in middle-aged and elderly populations: evidence from US and Chinese national population surveys.Lipids Health Dis. 2025 Apr 24;24(1):155. doi: 10.1186/s12944-025-02580-z. Lipids Health Dis. 2025. PMID: 40275392 Free PMC article.
References
-
- Katsimardou A, et al. Hypertension in metabolic syndrome: novel insights. Curr Hypertens Rev. 2020;16(1):12–18. - PubMed
-
- Wildman RP, et al. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: prevalence and correlates of 2 phenotypes among the US population (NHANES 1999–2004) Arch Intern Med. 2008;168(15):1617–1624. doi: 10.1001/archinte.168.15.1617. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
