

An updated review on the treatment for diversion colitis and pouchitis, with a focus on the utility of autologous fecal microbiota transplantation and its relationship with the intestinal microbiota
- PMID: 38966047
- PMCID: PMC11220330
- DOI: 10.12938/bmfh.2024-014
An updated review on the treatment for diversion colitis and pouchitis, with a focus on the utility of autologous fecal microbiota transplantation and its relationship with the intestinal microbiota
Abstract
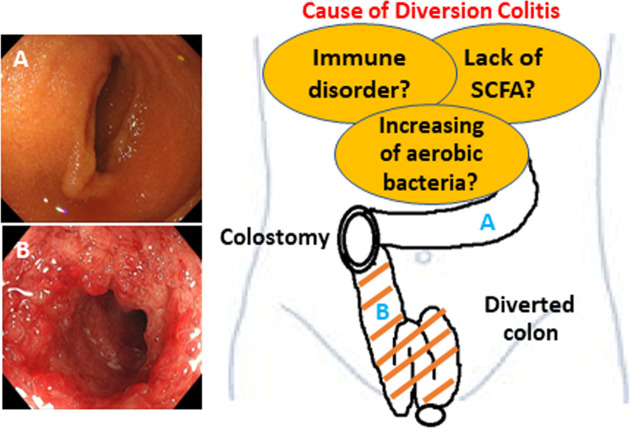
Diversion colitis (DC) is characterized by mucosal inflammation in the defunctioned segment of the colon following a colostomy or ileostomy. The major causes of DC are an increase in the number of aerobic bacteria, a lack of short-chain fatty acids (SCFAs), and immune disorders in the diverted colon. However, its exact pathogenesis remains unknown. Various treatment strategies for DC have been explored, although none have been definitively established. Treatment approaches such as SCFAs, 5-aminosalicylic acid enemas, steroid enemas, and irrigation with fibers have been attempted, yielding various degrees of efficacies in mitigating mucosal inflammation. However, only individual case reports demonstrating the limited effect of the following therapies have been published: leukocytapheresis, dextrose (hypertonic glucose) spray, infliximab, an elemental diet, and coconut oil. The usefulness of probiotics for treating DC has recently been reported. Furthermore, fecal microbiota transplantation (FMT) has emerged as a promising treatment for DC. This review provides an update on the treatment strategies of DC, with a particular focus on FMT and its relationship with the intestinal microbiota. FMT may become the first choice of treatment for some patients in the future because of its low medical costs, ease of use, and minimal side effects. Furthermore, FMT can also be used for postoperative DC prophylaxis.
Keywords: diversion colitis; fecal microbiota transplantation; ileitis; inflammatory bowel disease; microbiota; pouchitis; treatment.
©2024 BMFH Press.
Conflict of interest statement
The authors have no conflict of interest.
Figures
References
-
- Morson BC, Dawson IMP. 1972. Gastrointestinal pathology, 1st ed. Blackwellfic Publications, London.
-
- Glotzer DJ, Glick ME, Goldman H. 1981. Proctitis and colitis following diversion of the fecal stream. Gastroenterology 80: 438–441. - PubMed
-
- Korelitz BI, Cheskin LJ, Sohn N, Sommers SC. 1984. Proctitis after fecal diversion in Crohn’s disease and its elimination with reanastomosis: implications for surgical management. Report of four cases. Gastroenterology 87: 710–713. - PubMed
-
- Szczepkowski M, Kobus A, Borycka K. 2008. How to treat diversion colitis?—Current state of medical knowledge, own research and experience. Acta Chir Iugosl 55: 77–81. - PubMed
-
- Ma CK, Gottlieb C, Haas PA. 1990. Diversion colitis: a clinicopathologic study of 21 cases. Hum Pathol 21: 429–436. - PubMed