

Suprasellar Meningioma Classification: Endoscopic Transnasal Perspective
- PMID: 38966303
- PMCID: PMC11221907
- DOI: 10.1055/a-2070-8496
Suprasellar Meningioma Classification: Endoscopic Transnasal Perspective
Abstract
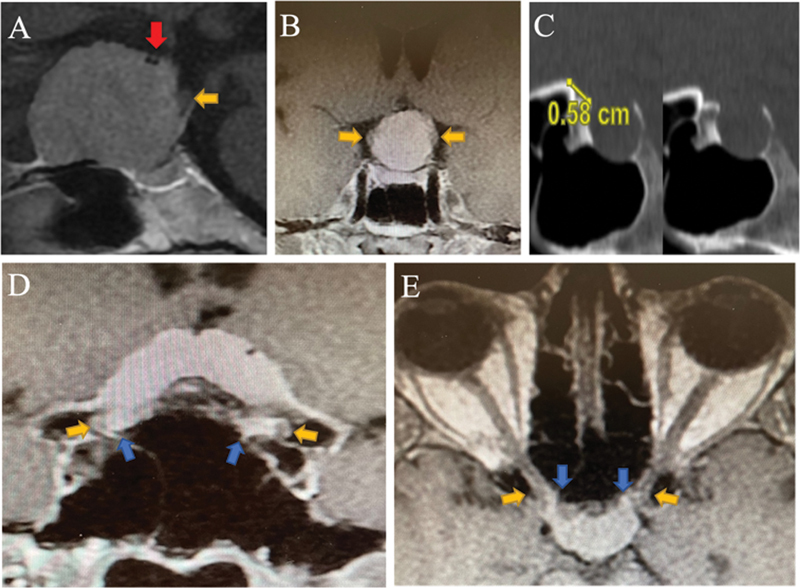
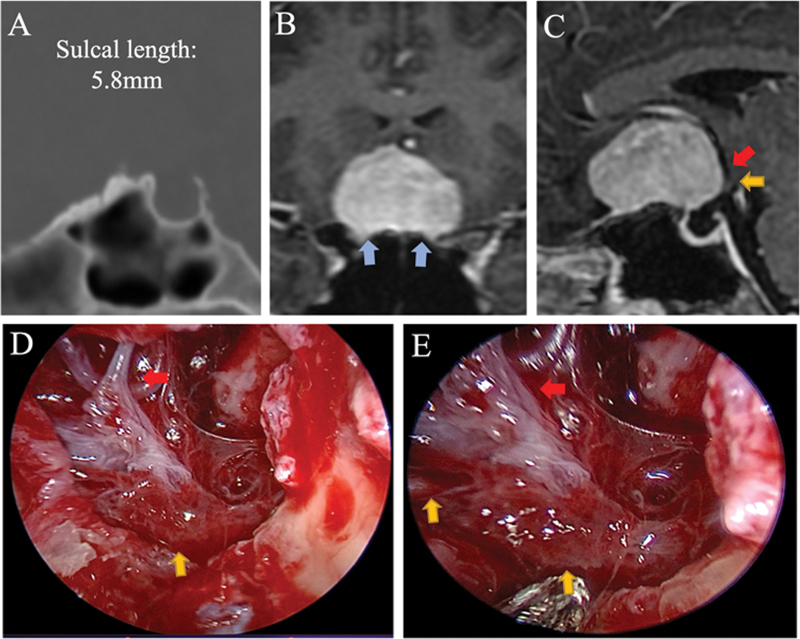
Objectives Midline suprasellar meningiomas include planum sphenoidale, tuberculum sellae, and diaphragma sellae meningiomas. Multiple classifications have been previously documented; however, they come with controversies and limitations, including those with surgical implications. The aim of this study was to classify suprasellar meningiomas based on their behavior toward the underlying bone and neurovascular structures. Methods Patients with newly diagnosed suprasellar meningiomas that underwent extended endoscopic transnasal approach between 2015 and 2021 were included in this study. The following parameters were evaluated: chiasmatic sulcus length, location of the optic chiasm and nerves, optic canal involvement, and vascular displacement. Results We identified 40 cases of midline suprasellar meningiomas, 1 diaphragma sellae meningioma (type A), 10 tuberculum sellae meningiomas (type B), 9 chiasmatic sulcus meningiomas (type C), and 10 planum sphenoidale meningiomas (type D). Asymmetrical visual complaints were most common in chiasmatic sulcus meningiomas, followed by tuberculum sellae meningiomas (66 and 50%, respectively). Chiasmatic sulcus meningiomas showed increased separation between the optic chiasm and the A1/A2 complex (8.9 mm) compared with tuberculum sellae (2.7 mm) and planum sphenoidale (1.9 mm) meningiomas. Compared with other types, increased chiasmatic sulcus length was observed in chiasmatic sulcus meningiomas. Conclusion Preoperative evaluation of bone involvement and tumor relation to neurovascular structures can be used to classify suprasellar meningiomas. Chiasmatic sulcus meningioma is a distinct subtype of suprasellar meningiomas. Its unique behavior toward nearby neurovascular structures could be of surgical value during tumor resection.
Keywords: chiasmatic sulcus; meningioma; suprasellar.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures




References
-
- DeMonte F. Surgical treatment of anterior basal meningiomas. J Neurooncol. 1996;29(03):239–248. - PubMed
-
- Al-Mefty O, Holoubi A, Rifai A, Fox J L. Microsurgical removal of suprasellar meningiomas. Neurosurgery. 1985;16(03):364–372. - PubMed
-
- Kwancharoen R, Blitz A M, Tavares F, Caturegli P, Gallia G L, Salvatori R. Clinical features of sellar and suprasellar meningiomas. Pituitary. 2014;17(04):342–348. - PubMed
-
- Henderson F, Youngerman B E, Niogi S N et al.Endonasal transsphenoidal surgery for planum sphenoidale versus tuberculum sellae meningiomas. J Neurosurg. 2022;138(05):1338–1346. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases