

Outcomes of Laparoscopic Suture Rectopexy Versus Laparoscopic Mesh Rectopexy: A Systematic Review and Meta-Analysis
- PMID: 38966481
- PMCID: PMC11223666
- DOI: 10.7759/cureus.61631
Outcomes of Laparoscopic Suture Rectopexy Versus Laparoscopic Mesh Rectopexy: A Systematic Review and Meta-Analysis
Abstract
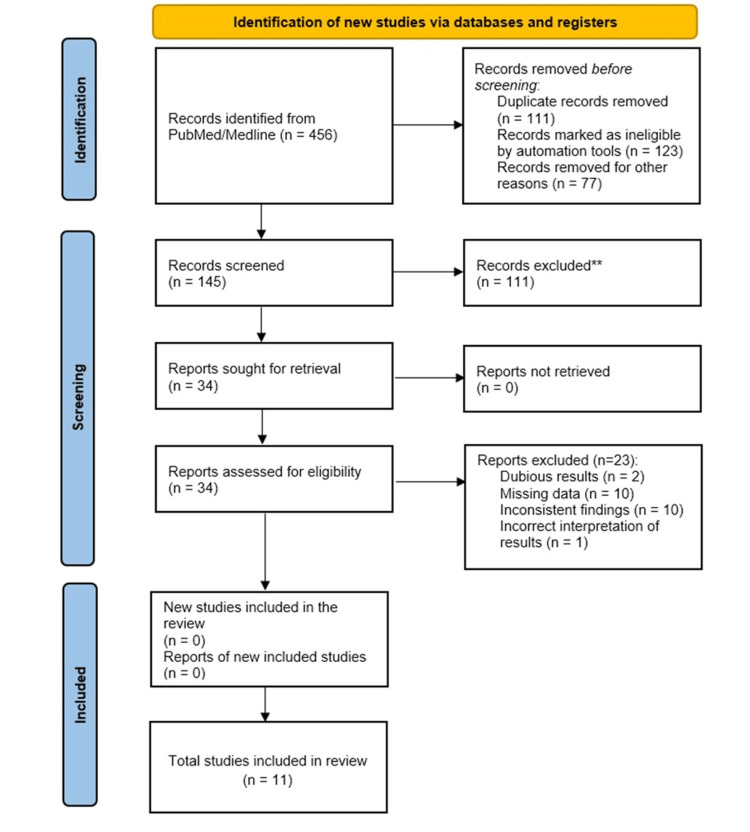
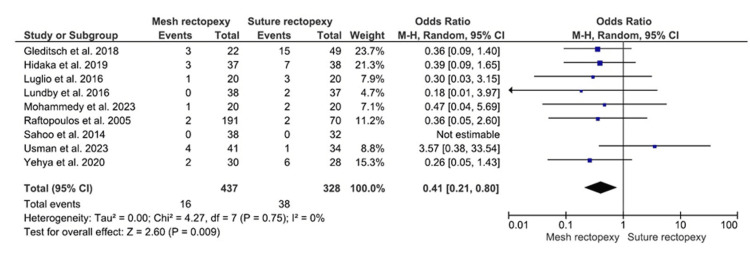
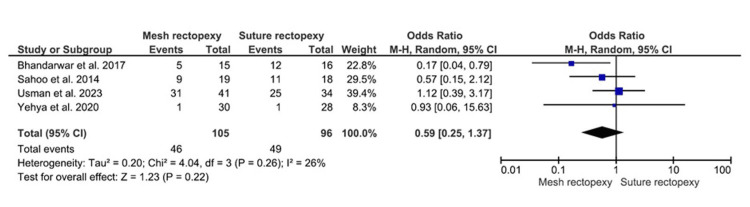
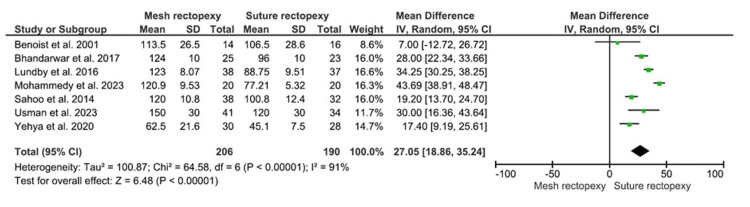
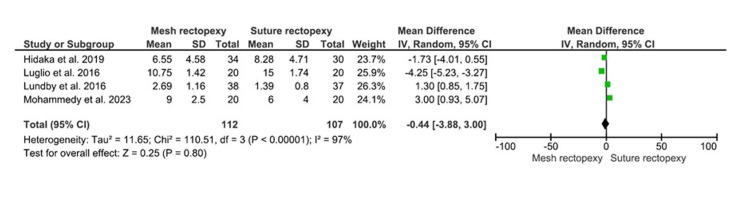
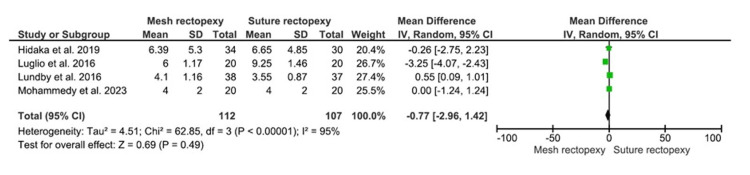
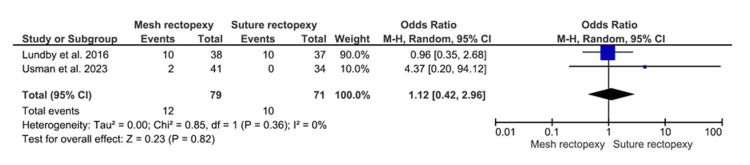
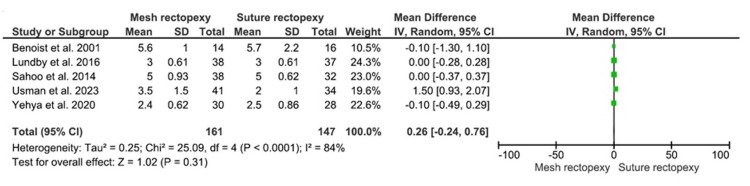
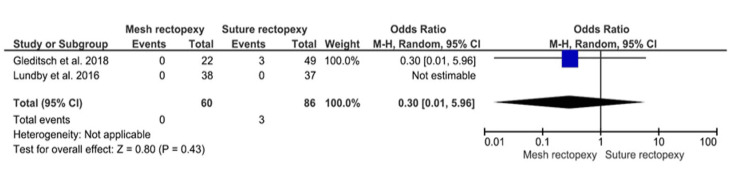
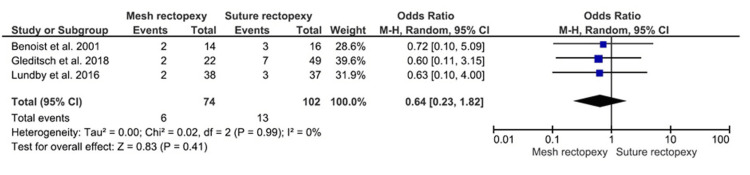
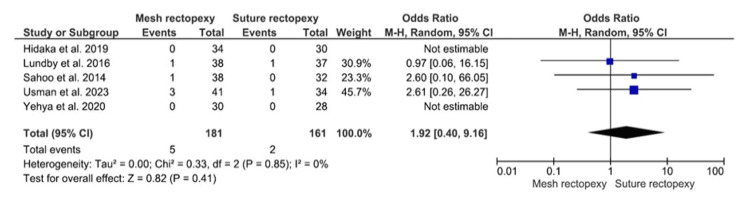
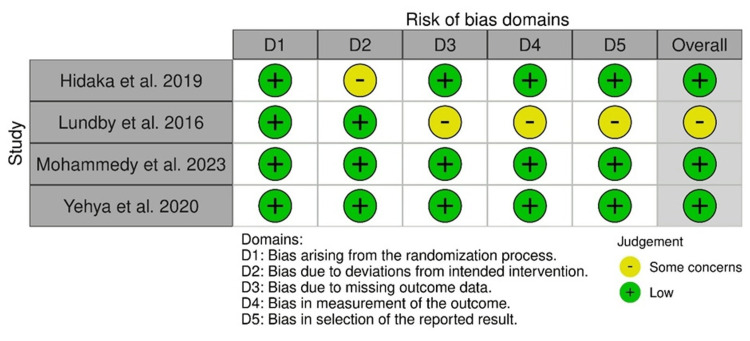
The contemporary literature provides conflicting evidence regarding the precedence of laparoscopic mesh rectopexy over laparoscopic suture rectopexy for full-thickness rectal prolapse. This study aimed to compare the clinical outcomes of mesh and suture rectopexy to improve the surgical management of complete rectal prolapse. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed to extract studies based on mesh versus suture rectopexy and published from 2001 to 2023. The articles of interest were obtained from PubMed Central, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Journal Storage (JSTOR), Web of Science, Embase, Scopus, and the Cochrane Library. The primary outcomes included rectal prolapse recurrence, constipation improvement, and operative time. The secondary endpoints included the Cleveland Clinic Constipation Score, Cleveland Clinic Incontinence Score, intraoperative bleeding, hospital stay duration, mortality, overall postoperative complications, and surgical site infection. A statistically significant low recurrence of rectal prolapse (odds ratio: 0.41, 95% confidence interval (CI) 0.21-0.80; p=0.009) and longer mean operative duration (mean difference: 27.05, 95% CI 18.86-35.24; p<0.00001) were observed in patients with mesh rectopexy versus suture rectopexy. Both study groups, however, had no significant differences in constipation improvement and all secondary endpoints (all p>0.05). The laparoscopic mesh rectopexy was associated with a low postoperative rectal prolapse recurrence and a longer operative duration compared to laparoscopic suture rectopexy. Prospective randomized controlled trials should further evaluate mesh and suture rectopexy approaches for postoperative outcomes to inform the surgical management of complete rectal prolapse.
Keywords: clinical outcomes; complete rectal prolapse; full-thickness rectal prolapse; laparoscopic rectopexy; mesh rectopexy; postoperative; suture rectopexy.
Copyright © 2024, Kumari et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Focus on abdominal rectopexy for full-thickness rectal prolapse: meta-analysis of literature.Tech Coloproctol. 2012 Feb;16(1):37-53. doi: 10.1007/s10151-011-0798-x. Epub 2011 Dec 15. Tech Coloproctol. 2012. PMID: 22170252 Review.
-
Laparoscopic Suture versus Mesh Rectopexy for the Treatment of Persistent Complete Rectal Prolapse in Children: A Comparative Randomized Study.Minim Invasive Surg. 2020 Jan 22;2020:3057528. doi: 10.1155/2020/3057528. eCollection 2020. Minim Invasive Surg. 2020. PMID: 32411460 Free PMC article.
-
Meta-analysis of laparoscopic mesh rectopexy versus posterior sutured rectopexy for management of complete rectal prolapse.Int J Colorectal Dis. 2021 Jul;36(7):1357-1366. doi: 10.1007/s00384-021-03883-0. Epub 2021 Feb 23. Int J Colorectal Dis. 2021. PMID: 33624175 Review.
-
Laparoscopic management of persistent complete rectal prolapse in children.J Pediatr Surg. 2010 Mar;45(3):533-9. doi: 10.1016/j.jpedsurg.2009.09.013. J Pediatr Surg. 2010. PMID: 20223316
-
Laparoscopic Versus Open Rectopexy for Rectal Prolapse: A Randomized Controlled Trial.Cureus. 2021 Mar 29;13(3):e14175. doi: 10.7759/cureus.14175. Cureus. 2021. PMID: 33936886 Free PMC article.
Cited by
-
Surgical approaches for complete rectal prolapse.World J Gastrointest Surg. 2025 Mar 27;17(3):102043. doi: 10.4240/wjgs.v17.i3.102043. World J Gastrointest Surg. 2025. PMID: 40162412 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources