

Bickerstaff Brainstem Encephalitis Presenting With Negative Anti-GM1 and Anti-GQ1B Antibodies
- PMID: 38966486
- PMCID: PMC11223585
- DOI: 10.7759/cureus.61653
Bickerstaff Brainstem Encephalitis Presenting With Negative Anti-GM1 and Anti-GQ1B Antibodies
Abstract
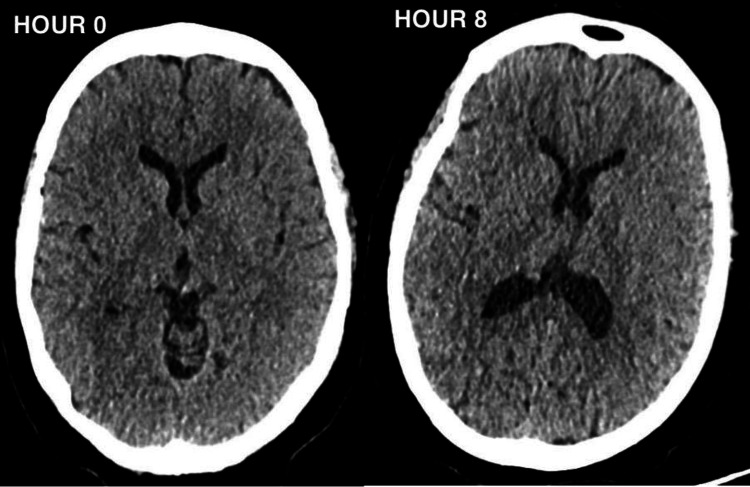
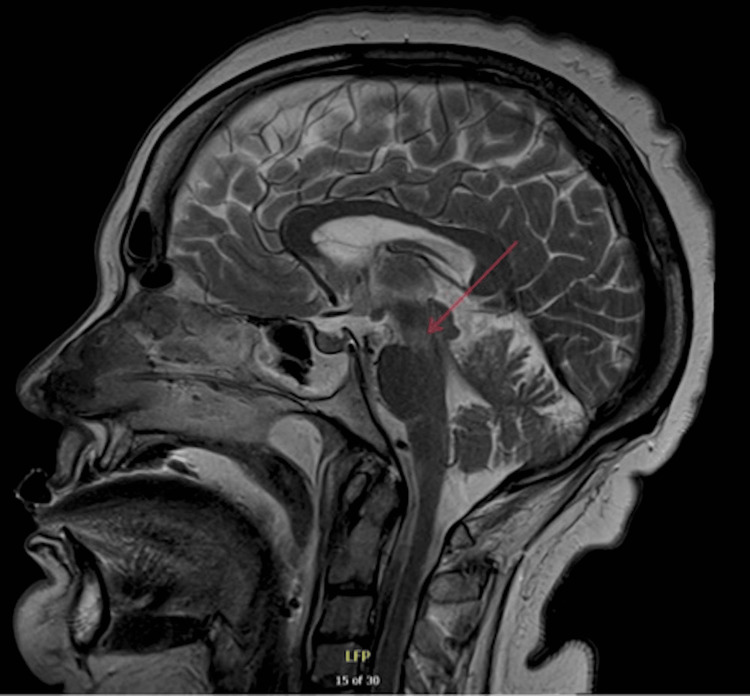
A woman in her 60s initially presented with rapid-onset left-sided hemiparesis with later development of slurred speech and left-sided facial droop. Despite ruling out common causes, her condition rapidly progressed with the development of bilateral proximal weakness, ophthalmoplegia, ataxia, and pyramidal signs eventually leading to a cardiorespiratory arrest. Extensive investigations, including computerised tomography (CT), magnetic resonance imaging (MRI), and lumbar puncture (LP), were negative for infectious or vascular aetiologies. Nerve conduction studies (NCS) revealed severe peripheral nerve damage, and despite a provisional diagnosis of Guillain-Barré Syndrome (GBS), the clinical picture aligned more with Bickerstaff Brainstem Encephalitis (BBE) given the central nervous system (CNS) involvement, despite negative anti-GM1 and anti-GQ1b autoantibodies. Treatment involved ventilatory support, immunoglobulins, and steroids. This case report describes a rare and challenging presentation of BBE and reminds clinicians to have a systematic approach to a patient presenting with rapid onset neurological symptoms and that BBE is a clinical diagnosis.
Keywords: autoimmune neuromuscular disease; intensive care medicine; invasive mechanical ventilation; neuro-critical care; neurology and critical care.
Copyright © 2024, Warcup et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
[Clinical features of 19 children with Bickerstaff brainstem encephalitis].Zhonghua Er Ke Za Zhi. 2019 May 2;57(5):363-367. doi: 10.3760/cma.j.issn.0578-1310.2019.05.009. Zhonghua Er Ke Za Zhi. 2019. PMID: 31060129 Chinese.
-
Bickerstaff Brainstem Encephalitis and overlapping Guillain-Barré syndrome in children: Report of two cases and review of the literature.Eur J Paediatr Neurol. 2019 Jan;23(1):43-52. doi: 10.1016/j.ejpn.2018.11.008. Epub 2018 Nov 20. Eur J Paediatr Neurol. 2019. PMID: 30502045 Review.
-
Miller Fisher syndrome, Bickerstaff brainstem encephalitis and Guillain-Barré syndrome overlap with persistent non-demyelinating conduction blocks: a case report.BMC Neurol. 2018 Jul 21;18(1):101. doi: 10.1186/s12883-018-1104-6. BMC Neurol. 2018. PMID: 30031375 Free PMC article.
-
Anti-ganglioside complex antibody profiles in a recurrent complicated case of GQ1b-seronegative miller fisher syndrome and Bickerstaff brainstem encephalitis: a case report.BMC Neurol. 2018 May 23;18(1):72. doi: 10.1186/s12883-018-1077-5. BMC Neurol. 2018. PMID: 29792178 Free PMC article.
-
Bickerstaff encephalitis in childhood: a review of 74 cases in the literature from 1951 to today.Front Neurol. 2024 Mar 12;15:1387505. doi: 10.3389/fneur.2024.1387505. eCollection 2024. Front Neurol. 2024. PMID: 38533411 Free PMC article. Review.
References
-
- Bickerstaff's brainstem encephalitis: clinical features of 62 cases and a subgroup associated with Guillain-Barré syndrome. Odaka M, Yuki N, Yamada M, Koga M, Takemi T, Hirata K, Kuwabara S. Brain. 2003;126:2279–2290. - PubMed
-
- Bickerstaff brainstem encephalitis and Fisher syndrome: anti-GQ1b antibody syndrome. Shahrizaila N, Yuki N. J Neurol Neurosurg Psychiatry. 2013;84:576–583. - PubMed
Publication types
LinkOut - more resources
Full Text Sources