

Measuring the Direct Medical Costs of Hospital-Onset Infections Using an Analogy Costing Framework
- PMID: 38967909
- PMCID: PMC11405445
- DOI: 10.1007/s40273-024-01400-z
Measuring the Direct Medical Costs of Hospital-Onset Infections Using an Analogy Costing Framework
Abstract
Background: The majority of recent estimates on the direct medical cost attributable to hospital-onset infections (HOIs) has focused on device- or procedure-associated HOIs. The attributable costs of HOIs that are not associated with device use or procedures have not been extensively studied.
Objective: We developed simulation models of attributable cost for 16 HOIs and estimated the total direct medical cost, including nondevice-related HOIs in the USA for 2011 and 2015.
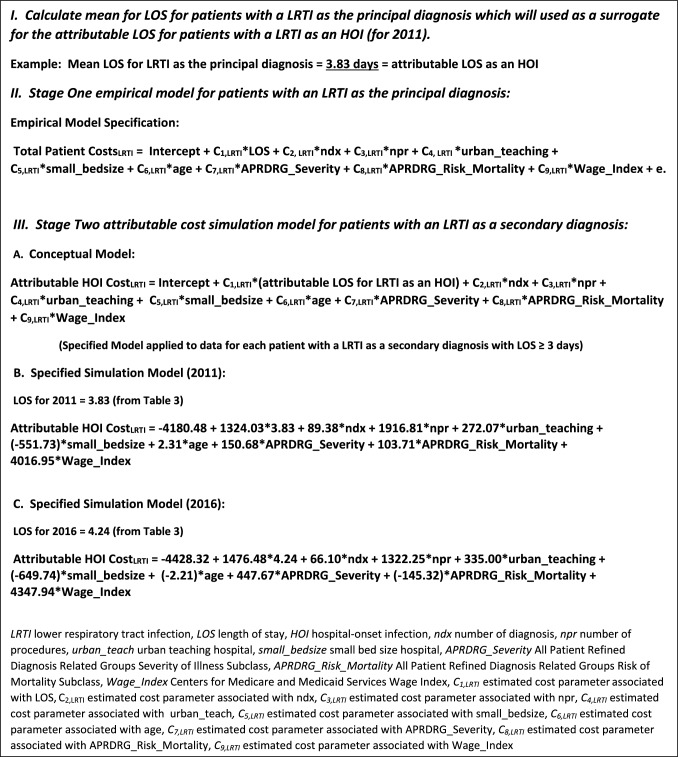
Data and methods: We used total discharge costs associated with HOI-related hospitalization from the National Inpatient Sample and applied an analogy costing methodology to develop simulation models of the costs attributable to HOIs. The mean attributable cost estimate from the simulation analysis was then multiplied by previously published estimates of the number of HOIs for 2011 and 2015 to generate national estimates of direct medical costs.
Results: After adjusting all estimates to 2017 US dollars, attributable cost estimates for select nondevice-related infections attributable cost estimates ranged from $7661 for ear, eye, nose, throat, and mouth (EENTM) infections to $27,709 for cardiovascular system infections in 2011; and from $8394 for EENTM to $26,445 for central nervous system infections in 2016 (based on 2015 incidence data). The national direct medical costs for all HOIs were $14.6 billion in 2011 and $12.1 billion in 2016. Nondevice- and nonprocedure-associated HOIs comprise approximately 26-28% of total HOI costs.
Conclusion: Results suggest that nondevice- and nonprocedure-related HOIs result in considerable costs to the healthcare system.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Estimation of Direct Healthcare Costs of Fungal Diseases in the United States.Clin Infect Dis. 2019 May 17;68(11):1791-1797. doi: 10.1093/cid/ciy776. Clin Infect Dis. 2019. PMID: 30204844 Free PMC article.
-
Assessment of Annual Cost of Substance Use Disorder in US Hospitals.JAMA Netw Open. 2021 Mar 1;4(3):e210242. doi: 10.1001/jamanetworkopen.2021.0242. JAMA Netw Open. 2021. PMID: 33666661 Free PMC article.
-
Economic costs of diabetes in the US in 2002.Diabetes Care. 2003 Mar;26(3):917-32. doi: 10.2337/diacare.26.3.917. Diabetes Care. 2003. PMID: 12610059
-
The attributable cost of catheter-associated urinary tract infections in the United States: A systematic review.Am J Infect Control. 2018 Jul;46(7):751-757. doi: 10.1016/j.ajic.2018.01.015. Epub 2018 Feb 22. Am J Infect Control. 2018. PMID: 29478760
-
Costs of Invasive Meningococcal Disease: A Global Systematic Review.Pharmacoeconomics. 2018 Oct;36(10):1201-1222. doi: 10.1007/s40273-018-0679-5. Pharmacoeconomics. 2018. PMID: 29948965
References
-
- Department of Health and Human Services (HHS). National Action Plan to Prevent Health Care-Associated Infections: Road Map to Elimination. 2013. https://health.gov/hcq/prevent-hai-action-plan.asp. Accessed on Sep 30, 2022.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
