

Comparing ventriculoatrial and ventriculopleural shunts in pediatric hydrocephalus: a Hydrocephalus Clinical Research Network study
- PMID: 38968629
- PMCID: PMC11244699
- DOI: 10.3171/2024.5.PEDS2469
Comparing ventriculoatrial and ventriculopleural shunts in pediatric hydrocephalus: a Hydrocephalus Clinical Research Network study
Abstract
Objective: When the peritoneal cavity cannot serve as the distal shunt terminus, nonperitoneal shunts, typically terminating in the atrium or pleural space, are used. The comparative effectiveness of these two terminus options has not been evaluated. The authors directly compared shunt survival and complication rates for ventriculoatrial (VA) and ventriculopleural (VPl) shunts in a pediatric cohort.
Methods: The Hydrocephalus Clinical Research Network Core Data Project was used to identify children ≤ 18 years of age who underwent either VA or VPl shunt insertion. The primary outcome was time to shunt failure. Secondary outcomes included distal site complications and frequency of shunt failure at 6, 12, and 24 months.
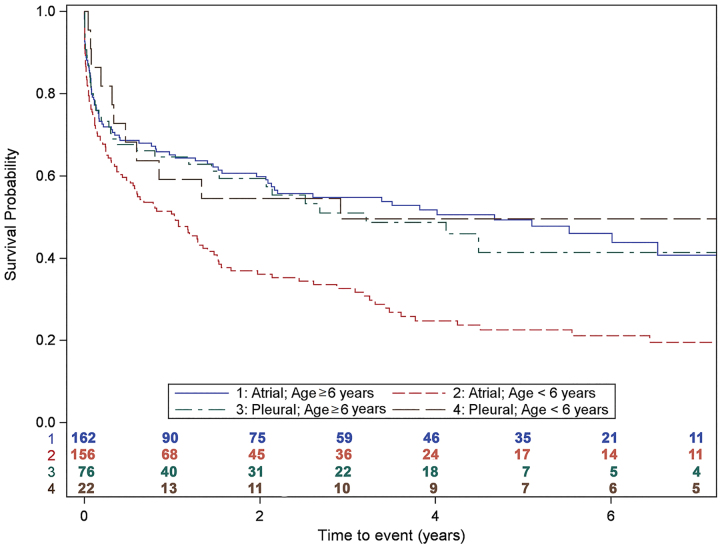
Results: The search criteria yielded 416 children from 14 centers with either a VA (n = 318) or VPl (n = 98) shunt, including those converted from ventriculoperitoneal shunts. Children with VA shunts had a lower median age at insertion (6.1 years vs 12.4 years, p < 0.001). Among those children with VA shunts, a hydrocephalus etiology of intraventricular hemorrhage (IVH) secondary to prematurity comprised a higher proportion (47.0% vs 31.2%) and myelomeningocele comprised a lower proportion (17.8% vs 27.3%) (p = 0.024) compared with those with VPl shunts. At 24 months, there was a higher cumulative number of revisions for VA shunts (48.6% vs 38.9%, p = 0.038). When stratified by patient age at shunt insertion, VA shunts in children < 6 years had the lowest shunt survival rate (p < 0.001, log-rank test). After controlling for age and etiology, multivariable analysis did not find that shunt type (VA vs VPl) was predictive of time to shunt failure. No differences were found in the cumulative frequency of complications (VA 6.0% vs VPl 9.2%, p = 0.257), but there was a higher rate of pneumothorax in the VPl cohort (3.1% vs 0%, p = 0.013).
Conclusions: Shunt survival was similar between VA and VPl shunts, although VA shunts are used more often, particularly in younger patients. Children < 6 years with VA shunts appeared to have the shortest shunt survival, which may be a result of the VA group having more cases of IVH secondary to prematurity; however, when age and etiology were included in a multivariable model, shunt location (atrium vs pleural space) was not associated with time to failure. The baseline differences between children treated with a VA versus a VPl shunt likely explain current practice patterns.
Keywords: Hydrocephalus Clinical Research Network; outcomes; pediatric; shunt failure; ventriculoatrial shunt; ventriculopleural shunt.
Conflict of interest statement
Dr. Limbrick reported being the CMO of Rhaeos Inc. outside the submitted work. Dr. Hauptman reported personal fees from Medtronic and BK Medical outside the submitted work. Dr. Jackson reported consulting fees from Integra LifeSciences outside the submitted work.
Figures

References
-
- Symss NP, Oi S. Is there an ideal shunt? A panoramic view of 110 years in CSF diversions and shunt systems used for the treatment of hydrocephalus: from historical events to current trends. Childs Nerv Syst. 2015;31(2):191–202. - PubMed
-
- Vernet O, Campiche R, de Tribolet N. Long-term results after ventriculo-atrial shunting in children. Childs Nerv Syst. 1995;11(3):176–179. - PubMed
-
- Zhang J, Qu C, Wang Z, et al. Improved ventriculoatrial shunt for cerebrospinal fluid diversion after multiple ventriculoperitoneal shunt failures. Surg Neurol. 2009;72(suppl 1):S29–S34. - PubMed
-
- Gmeiner M, Wagner H, van Ouwerkerk WJR, Senker W, Holl K, Gruber A. Abdominal pseudocysts and peritoneal catheter revisions: surgical long-term results in pediatric hydrocephalus. World Neurosurg. 2018;111:e912–e920. - PubMed
