

Single-centre real-life observational study on mortality and outcomes: decompressive craniectomy and brain death in traumatic brain injury, haemorrhage, and other cerebral diseases
- PMID: 38969875
- PMCID: PMC11226498
- DOI: 10.1007/s00701-024-06170-3
Single-centre real-life observational study on mortality and outcomes: decompressive craniectomy and brain death in traumatic brain injury, haemorrhage, and other cerebral diseases
Abstract
Background: Decompressive hemicraniectomy (DHC) is used after severe brain damages with elevated, refractory intracranial pressure (ICP). In a non age-restricted population, mortality rates and long-term outcomes following DHC are still unclear. This study's objectives were to examine both, as well as to identify predictors of unfavourable outcomes.
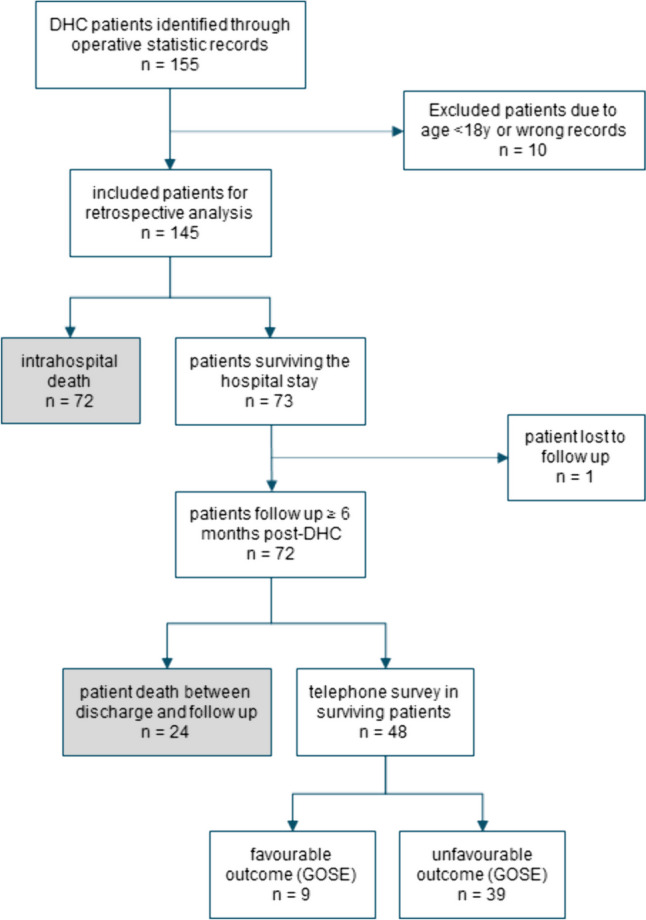
Methods: We undertook a retrospective observational analysis of patients aged 18 years and older who underwent DHC at the University Hospital of Bonn between 2018 and 2020, due to traumatic brain injury (TBI), haemorrhage, tumours or infections. Patient outcomes were assessed by conducting telephone interviews, utilising questionnaires for modified Rankin Scale (mRS) and extended Glasgow Outcome scale (GOSE). We evaluated the health-related quality of life using the EuroQol (EQ-5D-5L) scale.
Results: A total of 144 patients with a median age of 58.5 years (range: 18 to 85 years) were evaluated. The mortality rate was 67%, with patients passing away at a median of 6.0 days (IQR [1.9-37.6]) after DHC. Favourable outcomes, as assessed by the mRS and GOSE were observed in 10.4% and 6.3% of patients, respectively. Cox regression analysis revealed a 2.0% increase in the mortality risk for every year of age (HR = 1.017; 95% CI [1.01-1.03]; p = 0.004). Uni- and bilateral fixed pupils were associated with a 1.72 (95% CI [1.03-2.87]; p = 0.037) and 3.97 (95% CI [2.44-6.46]; p < 0.001) times higher mortality risk, respectively. ROC-analysis demonstrated that age and pupillary reactivity predicted 6-month mortality with an AUC of 0.77 (95% CI [0.69-0.84]). The only parameter significantly associated with a better quality of life was younger age.
Conclusions: Following DHC, mortality remains substantial, and favourable outcomes occur rarely. Particularly in elderly patients and in the presence of clinical signs of herniation, mortality rates are notably elevated. Hence, the indication for DHC should be set critically.
Keywords: Brain Death; Decompressive Craniectomy; Intracerebral Haemorrhage; Intracranial Pressure; Traumatic Brain Injury.
© 2024. The Author(s).
Conflict of interest statement
IS, EG, HV and MS report no competing interests.
Figures



References
-
- Al-Jishi A, Saluja RS, Al-Jehani H, Lamoureux J, Maleki M, Marcoux J (2011) Primary or secondary decompressive craniectomy: different indication and outcome. Can J Neurol Sci 38:612–620 - PubMed
-
- Cooper DJ, Rosenfeld JV, Murray L, Arabi YM, Davies AR, D’Urso P, Kossmann T, Ponsford J, Seppelt I, Reilly P, Wolfe R (2011) Decompressive craniectomy in diffuse traumatic brain injury. N Engl J Med 364:1493–1502 - PubMed
-
- Cooper DJ, Rosenfeld JV, Murray L, Arabi YM, Davies AR, Ponsford J, Seppelt I, Reilly P, Wiegers E, Wolfe R (2020) Patient Outcomes at Twelve Months after Early Decompressive Craniectomy for Diffuse Traumatic Brain Injury in the Randomized DECRA Clinical Trial. J Neurotrauma 37:810–816 - PMC - PubMed
-
- Esquenazi Y, Savitz SI, El Khoury R, McIntosh MA, Grotta JC, Tandon N (2015) Decompressive hemicraniectomy with or without clot evacuation for large spontaneous supratentorial intracerebral hemorrhages. Clin Neurol Neurosurg 128:117–122 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
