

Phenogrouping heart failure with preserved or mildly reduced ejection fraction using electronic health record data
- PMID: 38969974
- PMCID: PMC11229019
- DOI: 10.1186/s12872-024-03987-9
Phenogrouping heart failure with preserved or mildly reduced ejection fraction using electronic health record data
Abstract
Background: Heart failure (HF) with preserved or mildly reduced ejection fraction includes a heterogenous group of patients. Reclassification into distinct phenogroups to enable targeted interventions is a priority. This study aimed to identify distinct phenogroups, and compare phenogroup characteristics and outcomes, from electronic health record data.
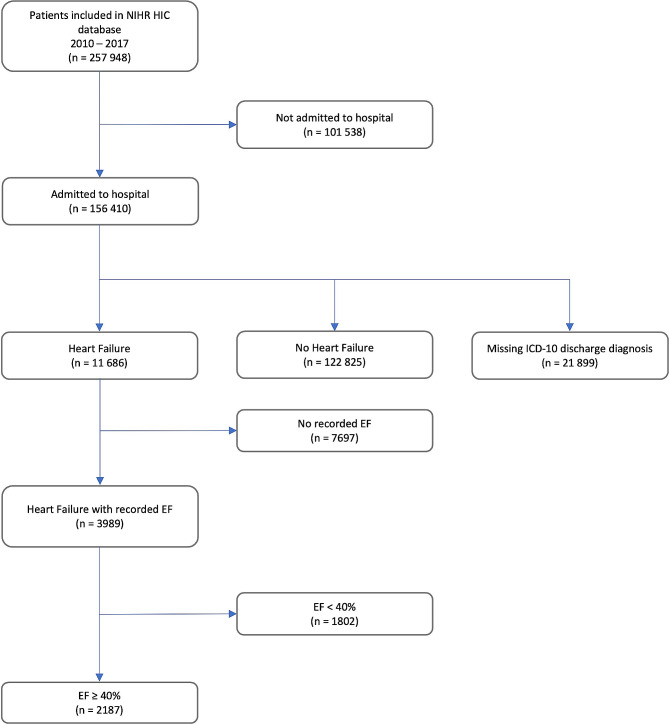
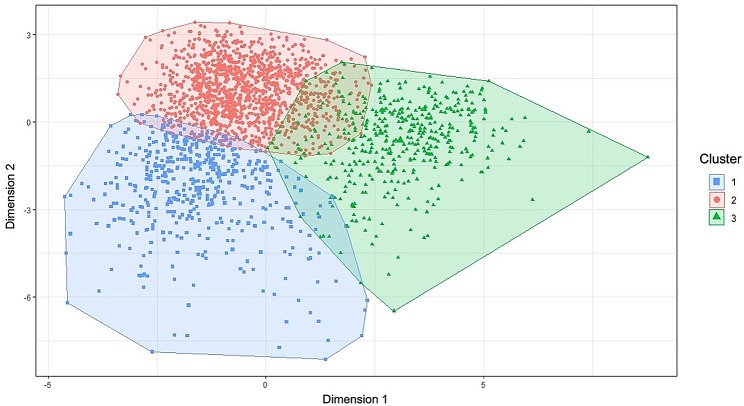
Methods: 2,187 patients admitted to five UK hospitals with a diagnosis of HF and a left ventricular ejection fraction ≥ 40% were identified from the NIHR Health Informatics Collaborative database. Partition-based, model-based, and density-based machine learning clustering techniques were applied. Cox Proportional Hazards and Fine-Gray competing risks models were used to compare outcomes (all-cause mortality and hospitalisation for HF) across phenogroups.
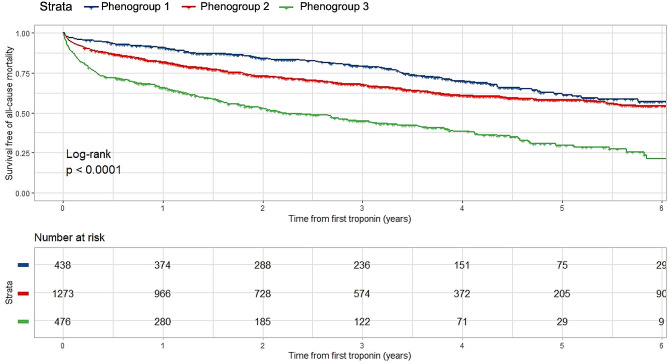
Results: Three phenogroups were identified: (1) Younger, predominantly female patients with high prevalence of cardiometabolic and coronary disease; (2) More frail patients, with higher rates of lung disease and atrial fibrillation; (3) Patients characterised by systemic inflammation and high rates of diabetes and renal dysfunction. Survival profiles were distinct, with an increasing risk of all-cause mortality from phenogroups 1 to 3 (p < 0.001). Phenogroup membership significantly improved survival prediction compared to conventional factors. Phenogroups were not predictive of hospitalisation for HF.
Conclusions: Applying unsupervised machine learning to routinely collected electronic health record data identified phenogroups with distinct clinical characteristics and unique survival profiles.
Keywords: Electronic health records; Heart failure with preserved or mildly reduced ejection fraction; Machine learning.
© 2024. The Author(s).
Conflict of interest statement
CAM has participated on advisory boards/consulted for AstraZeneca, Boehringer Ingelheim and Lilly Alliance, Novartis and PureTech Health, serves as an advisor for HAYA Therapeutics, has received speaker fees from AstraZeneca, Boehringer Ingelheim and Novo Nordisk, conference attendance support from AstraZeneca, and research support from Amicus Therapeutics, AstraZeneca, Guerbet Laboratories Limited, Roche and Univar Solutions B.V.
Figures
Similar articles
-
Heart failure with preserved ejection fraction phenogroup classification using machine learning.ESC Heart Fail. 2023 Jun;10(3):2019-2030. doi: 10.1002/ehf2.14368. Epub 2023 Apr 12. ESC Heart Fail. 2023. PMID: 37051638 Free PMC article.
-
Clinical Phenogroups in Heart Failure With Preserved Ejection Fraction: Detailed Phenotypes, Prognosis, and Response to Spironolactone.JACC Heart Fail. 2020 Mar;8(3):172-184. doi: 10.1016/j.jchf.2019.09.009. Epub 2020 Jan 8. JACC Heart Fail. 2020. PMID: 31926856 Free PMC article. Clinical Trial.
-
Characteristics, prognosis and treatment response in distinct phenogroups of heart failure with preserved ejection fraction.Int J Cardiol. 2021 Jan 15;323:148-154. doi: 10.1016/j.ijcard.2020.08.065. Epub 2020 Aug 26. Int J Cardiol. 2021. PMID: 32860842
-
Atrial fibrillation and risk of adverse outcomes in heart failure with reduced, mildly reduced, and preserved ejection fraction: A systematic review and meta-analysis.J Cardiovasc Electrophysiol. 2024 Apr;35(4):715-726. doi: 10.1111/jce.16209. Epub 2024 Feb 13. J Cardiovasc Electrophysiol. 2024. PMID: 38348517
-
Outcomes of heart failure with preserved ejection fraction in a Southeast Asian cohort.J Cardiovasc Med (Hagerstown). 2015 Sep;16(9):583-90. doi: 10.2459/JCM.0000000000000100. J Cardiovasc Med (Hagerstown). 2015. PMID: 25022929 Review.
References
-
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2021;42(36):3599–726. doi: 10.1093/eurheartj/ehab368. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
