

Highly extensile approach for comminuted ulna coronoid process fractures with mini-plate fixation: a case series of 31 patients
- PMID: 38970051
- PMCID: PMC11225124
- DOI: 10.1186/s12891-024-07637-1
Highly extensile approach for comminuted ulna coronoid process fractures with mini-plate fixation: a case series of 31 patients
Abstract
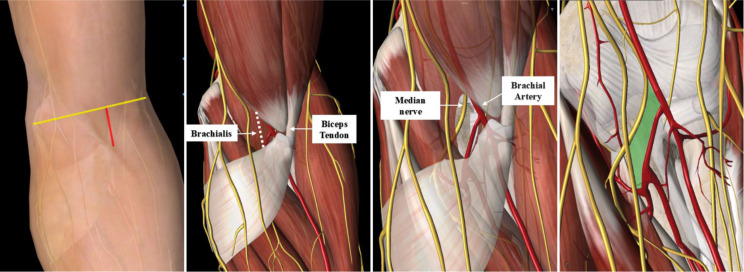
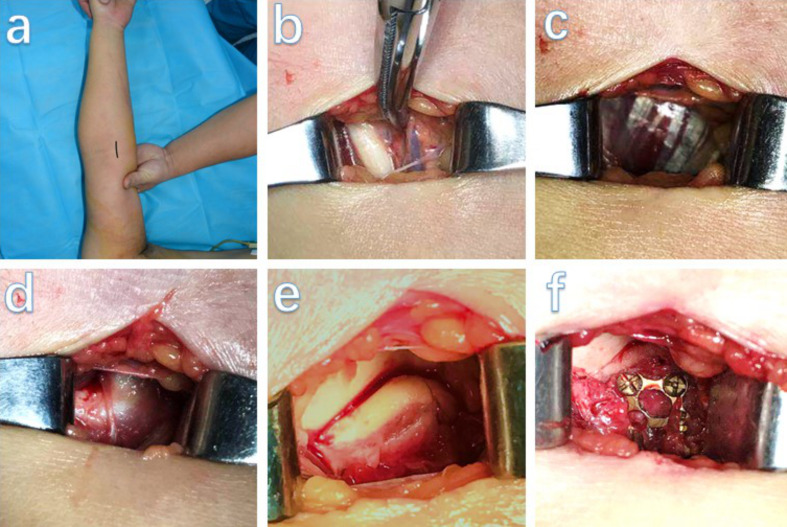
Background: For the treatment of coronoid process fractures, medial, lateral, anterior, anteromedial, and posterior approaches have been increasingly reported; however, there is no general consensus on the method of fixation of coronal fractures. Here, we present a highly-extensile minimally invasive approach to treat coronoid process fractures using a mini-plate that can achieve anatomic reduction, stable fixation, and anterior capsular repair. Further, the study aimed to determine the complication rate of the anterior minimally invasive approach and to evaluate functional and clinical patient-reported outcomes during follow-up.
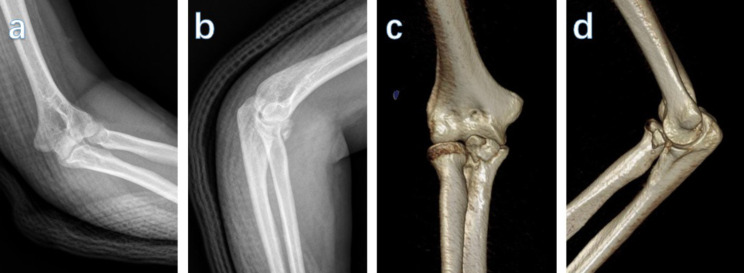
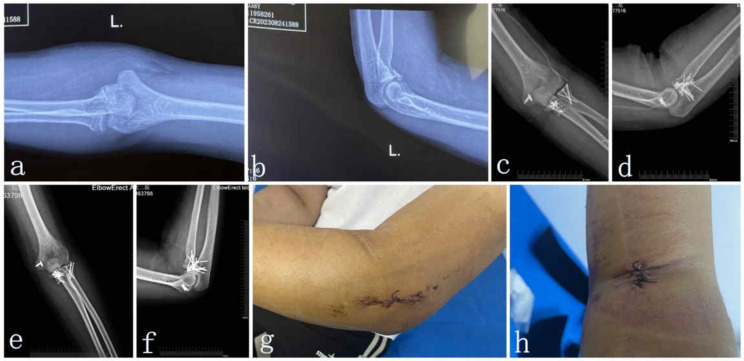
Methods: Thirty-one patients diagnosed with coronoid fractures accompanied with a "terrible triad" or posteromedial rotational instability between April 2012 and October 2018 were included in the analysis. Anatomical reduction and mini-plate fixation of coronoid fractures were performed using an anterior minimally invasive approach. Patient-reported outcomes were evaluated using the Mayo Elbow Performance Index (MEPI) score, range of motion (ROM), and the visual analog score (VAS). The time of fracture healing and complications were recorded.
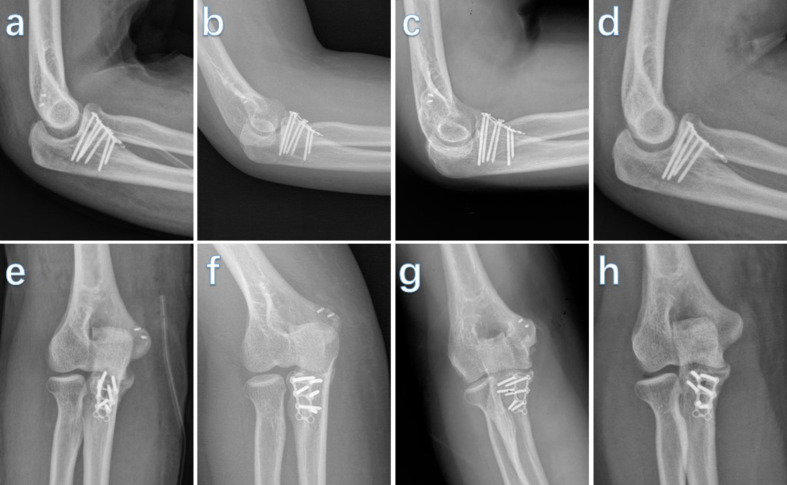
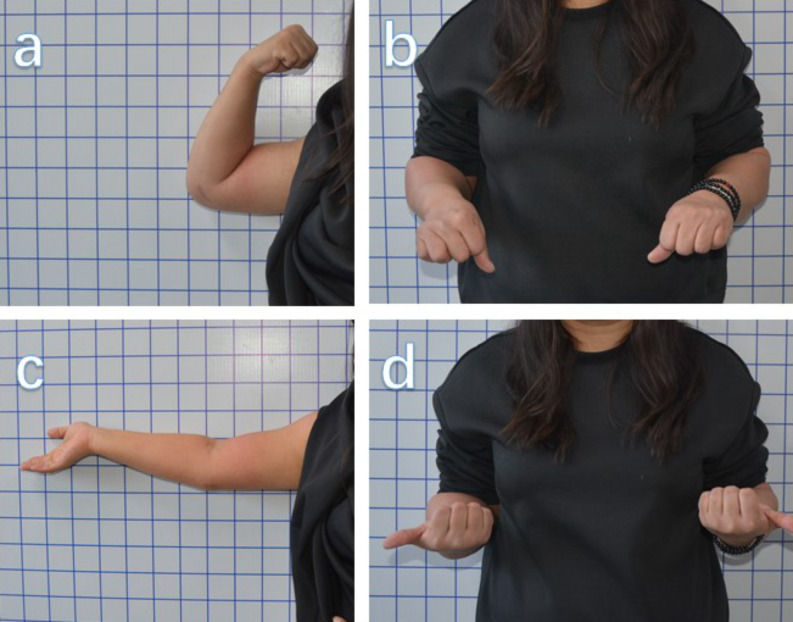
Results: The mean follow-up time was 26.7 months (range, 14-60 months). The average time to radiological union was 3.6 ± 1.3 months. During the follow-up period, the average elbow extension was 6.8 ± 2.9° while the average flexion was 129.6 ± 4.6°. According to Morrey's criteria, 26 (81%) elbows achieved a normal desired ROM. At the last follow-up, the mean MEPI score was 98 ± 3.3 points. There were no instances of elbow instability, elbow joint stiffness, subluxation or dislocation, infection, blood vessel complications, or nerve palsy. Overall, 10 elbows (31%) experienced heterotopic ossification.
Conclusion: An anterior minimally invasive approach allows satisfactory fixation of coronoid fractures while reducing incision complications due to over-dissection of soft tissue injuries. In addition, this incision does not compromise the soft tissue stability of the elbow joint and allows the patient a more rapid return to rehabilitation exercises.
Keywords: Anterior minimally invasive approach; Coronoid process fractures; Highly extensile approach; Mayo elbow performance index score; Mini-plate fixation.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Direct anterior approach for mini plate fixation of Regan-Morrey type II comminuted ulnar coronoid process fracture.J Orthop Surg (Hong Kong). 2019 Jan-Apr;27(1):2309499018825223. doi: 10.1177/2309499018825223. J Orthop Surg (Hong Kong). 2019. PMID: 30798735
-
Use of Mother-Child Screws in the Treatment of Coronoid Fractures in Terrible Triad Injury of the Elbow.Acta Chir Orthop Traumatol Cech. 2018;85(2):102-108. Acta Chir Orthop Traumatol Cech. 2018. PMID: 30295595 English.
-
[Effectiveness of improved elbow anteromedial approach in treatment of ulna coronoid process fracture].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2017 Dec 15;31(12):1409-1413. doi: 10.7507/1002-1892.201701091. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2017. PMID: 29806377 Free PMC article. Chinese.
-
Plate fixation through an anterior approach for coronoid process fractures: A retrospective case series and a literature review.Medicine (Baltimore). 2018 Sep;97(36):e12041. doi: 10.1097/MD.0000000000012041. Medicine (Baltimore). 2018. PMID: 30200084 Free PMC article. Review.
-
Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. Surgical technique.J Bone Joint Surg Am. 2005 Mar;87 Suppl 1(Pt 1):22-32. doi: 10.2106/JBJS.D.02933. J Bone Joint Surg Am. 2005. PMID: 15743844 Review.
Cited by
-
Treatment of the terrible triad of the elbow by olecranon osteotomy: a retrospective cohort study.PeerJ. 2024 Nov 15;12:e18469. doi: 10.7717/peerj.18469. eCollection 2024. PeerJ. 2024. PMID: 39559330 Free PMC article.
-
Superior outcome with anterolateral approach in treating O'Driscoll type II ulnar coronoid process fractures: a retrospective analysis.Am J Transl Res. 2025 Jan 15;17(1):440-449. doi: 10.62347/OUWK4004. eCollection 2025. Am J Transl Res. 2025. PMID: 39959191 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
