

Effectiveness of virtual and augmented reality for cardiopulmonary resuscitation training: a systematic review and meta-analysis
- PMID: 38970090
- PMCID: PMC11227211
- DOI: 10.1186/s12909-024-05720-8
Effectiveness of virtual and augmented reality for cardiopulmonary resuscitation training: a systematic review and meta-analysis
Abstract
Background: Virtual reality (VR) and augmented reality (AR) are emerging technologies that can be used for cardiopulmonary resuscitation (CPR) training. Compared to traditional face-to-face training, VR/AR-based training has the potential to reach a wider audience, but there is debate regarding its effectiveness in improving CPR quality. Therefore, we conducted a meta-analysis to assess the effectiveness of VR/AR training compared with face-to-face training.
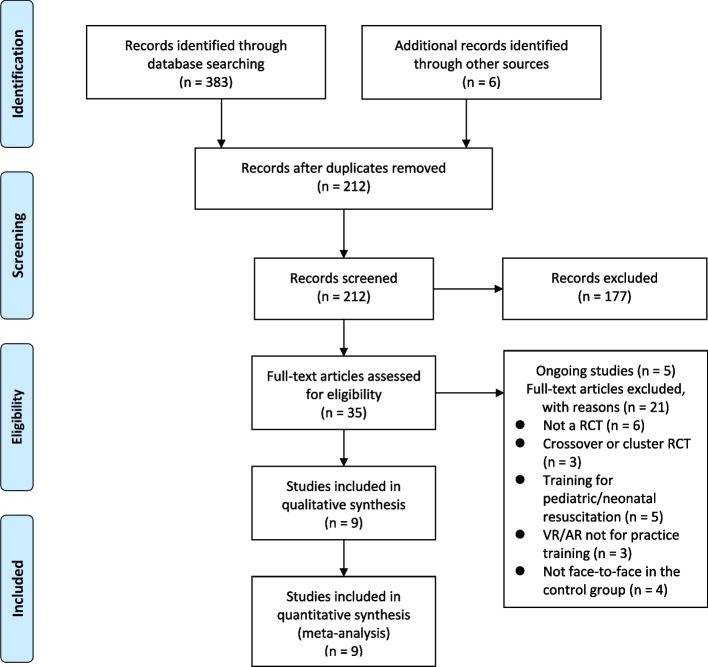
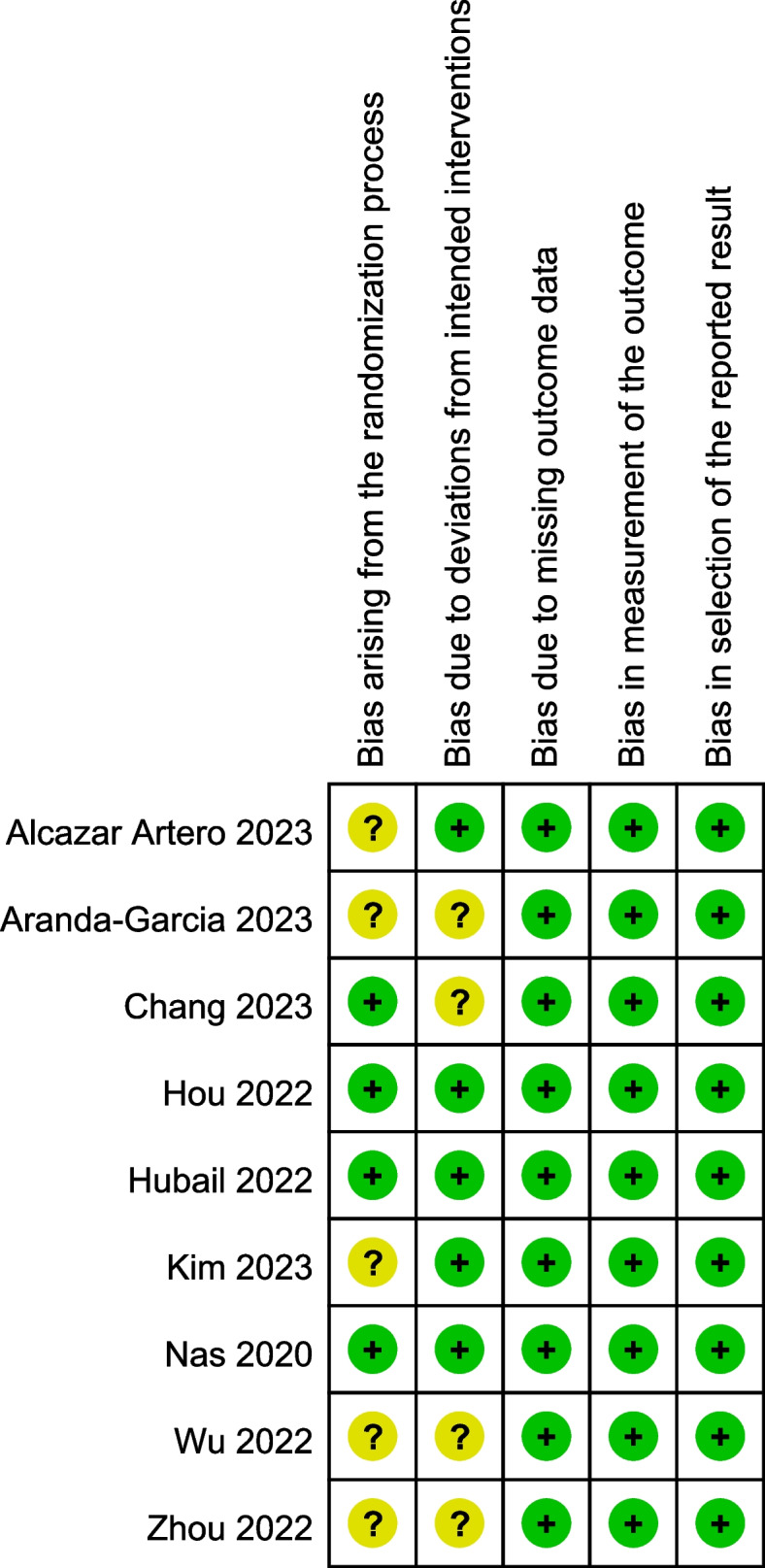
Methods: We searched PubMed, Embase, Cochrane Library, Web of Science, CINAHL, China National Knowledge Infrastructure, and Wanfang databases from the inception of these databases up until December 1, 2023, for randomized controlled trials (RCTs) comparing VR- and AR-based CPR training to traditional face-to-face training. Cochrane's tool for assessing bias in RCTs was used to assess the methodological quality of the included studies. We pooled the data using a random-effects model with Review Manager 5.4, and assessed publication bias with Stata 11.0.
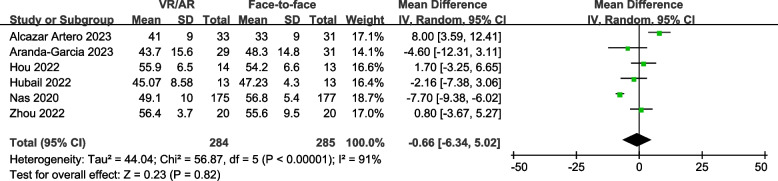
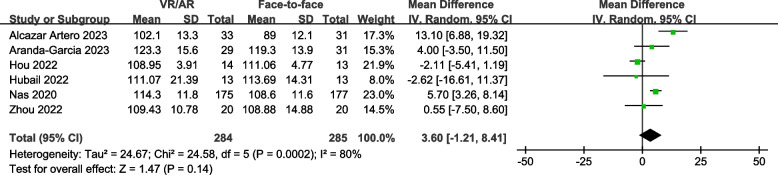
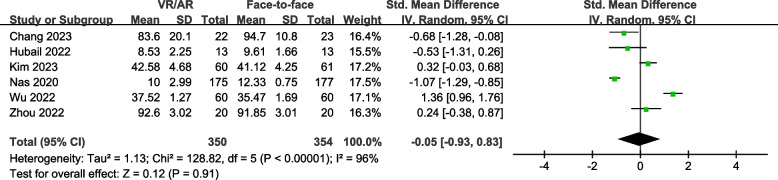
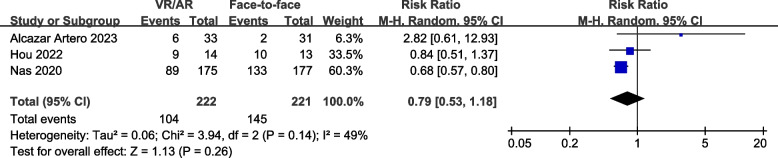
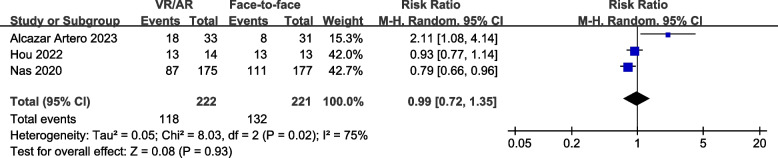
Results: Nine RCTs (involving 855 participants) were included, of which three were of low risk of bias. Meta-analyses showed no significant differences between VR/AR-based CPR training and face-to-face CPR training in terms of chest compression depth (mean difference [MD], -0.66 mm; 95% confidence interval [CI], -6.34 to 5.02 mm; P = 0.82), chest compression rate (MD, 3.60 compressions per minute; 95% CI, -1.21 to 8.41 compressions per minute; P = 0.14), overall CPR performance score (standardized mean difference, -0.05; 95% CI, -0.93 to 0.83; P = 0.91), as well as the proportion of participants meeting CPR depth criteria (risk ratio [RR], 0.79; 95% CI, 0.53 to 1.18; P = 0.26) and rate criteria (RR, 0.99; 95% CI, 0.72 to 1.35; P = 0.93). The Egger regression test showed no evidence of publication bias.
Conclusions: Our study showed evidence that VR/AR-based training was as effective as traditional face-to-face CPR training. Nevertheless, there was substantial heterogeneity among the included studies, which reduced confidence in the findings. Future studies need to establish standardized VR/AR-based CPR training protocols, evaluate the cost-effectiveness of this approach, and assess its impact on actual CPR performance in real-life scenarios and patient outcomes.
Trial registration: CRD42023482286.
Keywords: Augmented reality; Basic life support; Cardiopulmonary resuscitation; Meta-analysis; Systematic review; Virtual reality.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Effectiveness of extended reality technologies in cardiopulmonary resuscitation training: a bayesian network meta-analysis.BMC Emerg Med. 2025 Jun 7;25(1):94. doi: 10.1186/s12873-025-01256-2. BMC Emerg Med. 2025. PMID: 40483416 Free PMC article.
-
Effect of Face-to-Face vs Virtual Reality Training on Cardiopulmonary Resuscitation Quality: A Randomized Clinical Trial.JAMA Cardiol. 2020 Mar 1;5(3):328-335. doi: 10.1001/jamacardio.2019.4992. JAMA Cardiol. 2020. PMID: 31734702 Free PMC article. Clinical Trial.
-
Efficacy of virtual reality techniques in cardiopulmonary resuscitation training: protocol for a meta-analysis of randomised controlled trials and trial sequential analysis.BMJ Open. 2022 Feb 11;12(2):e058827. doi: 10.1136/bmjopen-2021-058827. BMJ Open. 2022. PMID: 35149577 Free PMC article.
-
Virtual reality simulation training for health professions trainees in gastrointestinal endoscopy.Cochrane Database Syst Rev. 2018 Aug 17;8(8):CD008237. doi: 10.1002/14651858.CD008237.pub3. Cochrane Database Syst Rev. 2018. PMID: 30117156 Free PMC article.
-
The Effects of Serious Games on Cardiopulmonary Resuscitation Training and Education: Systematic Review With Meta-Analysis of Randomized Controlled Trials.JMIR Serious Games. 2024 Feb 6;12:e52990. doi: 10.2196/52990. JMIR Serious Games. 2024. PMID: 38319697 Free PMC article. Review.
Cited by
-
Effectiveness of extended reality technologies in cardiopulmonary resuscitation training: a bayesian network meta-analysis.BMC Emerg Med. 2025 Jun 7;25(1):94. doi: 10.1186/s12873-025-01256-2. BMC Emerg Med. 2025. PMID: 40483416 Free PMC article.
-
Extended reality technologies in adult basic life support education: A scoping review.Resusc Plus. 2025 Mar 14;23:100927. doi: 10.1016/j.resplu.2025.100927. eCollection 2025 May. Resusc Plus. 2025. PMID: 40235926 Free PMC article. Review.
-
Technological innovations in layperson CPR education - A scoping review.Resusc Plus. 2025 Mar 5;23:100924. doi: 10.1016/j.resplu.2025.100924. eCollection 2025 May. Resusc Plus. 2025. PMID: 40212904 Free PMC article. Review.
-
Transforming anaesthesia education with extended reality: from preclinical training to independent clinical practice.Anaesth Rep. 2025 Jun 13;13(1):e70016. doi: 10.1002/anr3.70016. eCollection 2025 Jan-Jun. Anaesth Rep. 2025. PMID: 40520411 No abstract available.
References
-
- Yan S, Gan Y, Jiang N, Wang R, Chen Y, Luo Z, Zong Q, Chen S, Lv C. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis. Crit Care. 2020;24(1):61. doi: 10.1186/s13054-020-2773-2. - DOI - PMC - PubMed
-
- Malta HC, Kragholm K, Pearson DA, Tyson C, Monk L, Myers B, Nelson D, Dupre ME, Fosbol EL, Jollis JG, Strauss B, Anderson ML, McNally B, Granger CB. Association of bystander and first-responder intervention with survival after out-of-hospital cardiac arrest in North Carolina, 2010–2013. JAMA. 2015;314(3):255–264. doi: 10.1001/jama.2015.7938. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
