

Cardiovascular Magnetic Resonance Before Invasive Coronary Angiography in Suspected Non-ST-Segment Elevation Myocardial Infarction
- PMID: 38970595
- PMCID: PMC11512682
- DOI: 10.1016/j.jcmg.2024.05.007
Cardiovascular Magnetic Resonance Before Invasive Coronary Angiography in Suspected Non-ST-Segment Elevation Myocardial Infarction
Abstract
Background: In suspected non-ST-segment elevation myocardial infarction (NSTEMI), this presumed diagnosis may not hold true in all cases, particularly in patients with nonobstructive coronary arteries (NOCA). Additionally, in multivessel coronary artery disease, the presumed infarct-related artery may be incorrect.
Objectives: This study sought to assess the diagnostic utility of cardiac magnetic resonance (CMR) before invasive coronary angiogram (ICA) in suspected NSTEMI.
Methods: A total of 100 consecutive stable patients with suspected acute NSTEMI (70% male, age 62 ± 11 years) prospectively underwent CMR pre-ICA to assess cardiac function (cine), edema (T2-weighted imaging, T1 mapping), and necrosis/scar (late gadolinium enhancement). CMR images were interpreted blinded to ICA findings. The clinical care and ICA teams were blinded to CMR findings until post-ICA.
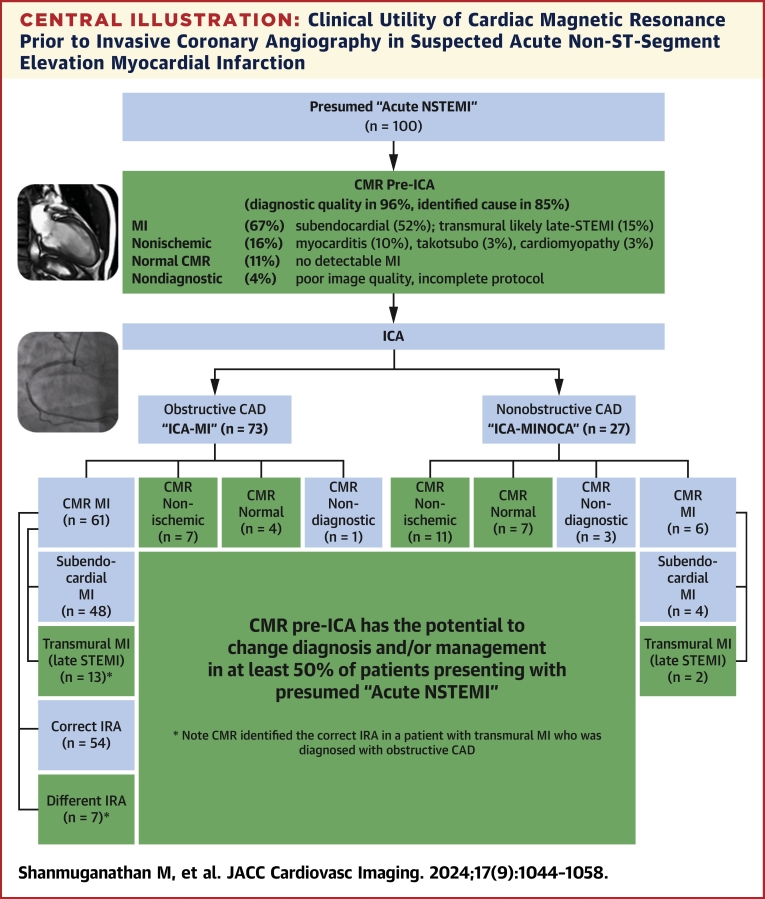
Results: Early CMR (median 33 hours postadmission and 4 hours pre-ICA) confirmed only 52% (52 of 100) of patients had subendocardial infarction, 15% transmural infarction, 18% nonischemic pathologies (myocarditis, takotsubo, and other forms of cardiomyopathies), and 11% normal CMR; 4% were nondiagnostic. Subanalyses according to ICA findings showed that, in patients with obstructive coronary artery disease (73 of 100), CMR confirmed only 84% (61 of 73) had MI, 10% (7 of 73) nonischemic pathologies, and 5% (4 of 73) normal. In patients with NOCA (27 of 100), CMR found MI in only 22% (6 of 27 true MI with NOCA), and reclassified the presumed diagnosis of NSTEMI in 67% (18 of 27: 11 nonischemic pathologies, 7 normal). In patients with CMR-MI and obstructive coronary artery disease (61 of 100), CMR identified a different infarct-related artery in 11% (7 of 61).
Conclusions: In patients presenting with suspected NSTEMI, a CMR-first strategy identified MI in 67%, nonischemic pathologies in 18%, and normal findings in 11%. Accordingly, CMR has the potential to affect at least 50% of all patients by reclassifying their diagnosis or altering their potential management.
Keywords: CMR; MINOCA; NSTEMI; acute coronary syndrome; early cardiac magnetic resonance; myocarditis.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The OxAMI study is supported by a British Heart Foundation (BHF) Centre of Research Excellence (CRE) Oxford (RE/13/1/30181), and the National Institute for Health Research Oxford Biomedical Research Centre. Dr Shanmuganathan has received funding from the Alison Brading Memorial Graduate Scholarship in Medical Science, Lady Margaret Hall, University of Oxford. Dr Burrage has received support from a British Heart Foundation Clinical Research Training Fellowship (FS/19/65/34692). Dr Gara has received a European Society of Cardiology, EACVI Research grant. Dr Piechnik has received support from the BHF CRE Oxford (RE/18/3/34214); and has patent authorship rights for U.S. patent 9285446 B2 (systems and methods for Shortened Look Locker Inversion Recovery [Sh-MOLLI] cardiac gated mapping of T1), granted March 15, 2016; intellectual properties are owned and managed by Oxford University Innovations. Dr Channon has received funding from a BHF Chair award (CH/16/1/32013). Dr Ferreira has received funding from the BHF, BHF CRE Oxford, and National Institute for Health Research Oxford Biomedical Research Center. The funders were not involved in the design and conduct of the study, in the collection, analysis, and interpretation of the data, and in the preparation, review, or approval of the manuscript. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures







References
-
- Amsterdam E.A., Wenger N.K., Brindis R.G., et al. 2014 AHA/ACC guideline for the management of patients with non–ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139–e228. - PubMed
-
- Bueno H. In: The ESC Textbook of Cardiovascular Medicine. James S., Camm A.J., Lüscher T.F., Maurer G., Serruys P.W., editors. Oxford University ress; 2018. Epidemiology of acute coronary syndromes. - DOI
-
- NICOR Myocardial Ischaemia/MINAP (Heart Attack audit) https://www.nicor.org.uk/national-cardiac-audit-programme/heart-attack-a...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
