

Guidelines for clinical evaluation of chronic kidney disease in early stages : AMED research on regulatory science of pharmaceuticals and medical devices
- PMID: 38970650
- PMCID: PMC11341658
- DOI: 10.1007/s10157-024-02514-6
Guidelines for clinical evaluation of chronic kidney disease in early stages : AMED research on regulatory science of pharmaceuticals and medical devices
Abstract
Background: For the development of pharmaceutical products in kidney field, appropriate surrogate endpoints which can predict long-term prognosis are needed as an alternative to hard endpoints, such as end-stage kidney disease. Though international workshop has proposed estimated glomerular filtration rate (GFR) slope reduction of 0.5-1.0 mL/min/1.73 m /year and 30% decrease in albuminuria/proteinuria as surrogate endpoints in early and advanced chronic kidney disease (CKD), it was not clear whether these are applicable to Japanese patients.
Methods: We analyzed J-CKD-DB and CKD-JAC, Japanese databases/cohorts of CKD patients, and J-DREAMS, a Japanese database of patients with diabetes mellitus to investigate the applicability of eGFR slope and albuminuria/proteinuria to the Japanese population. Systematic review on those endpoints was also conducted including the results of clinical trials published after the above proposal.
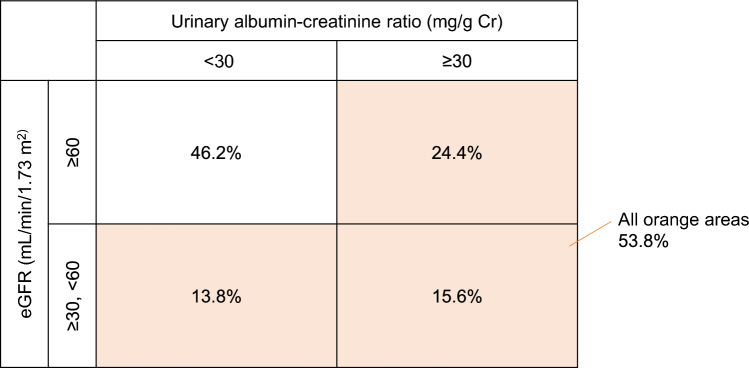
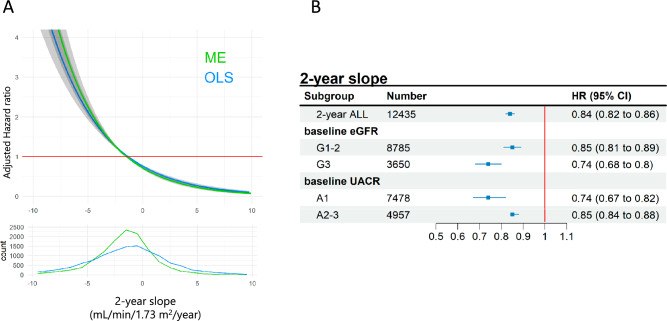
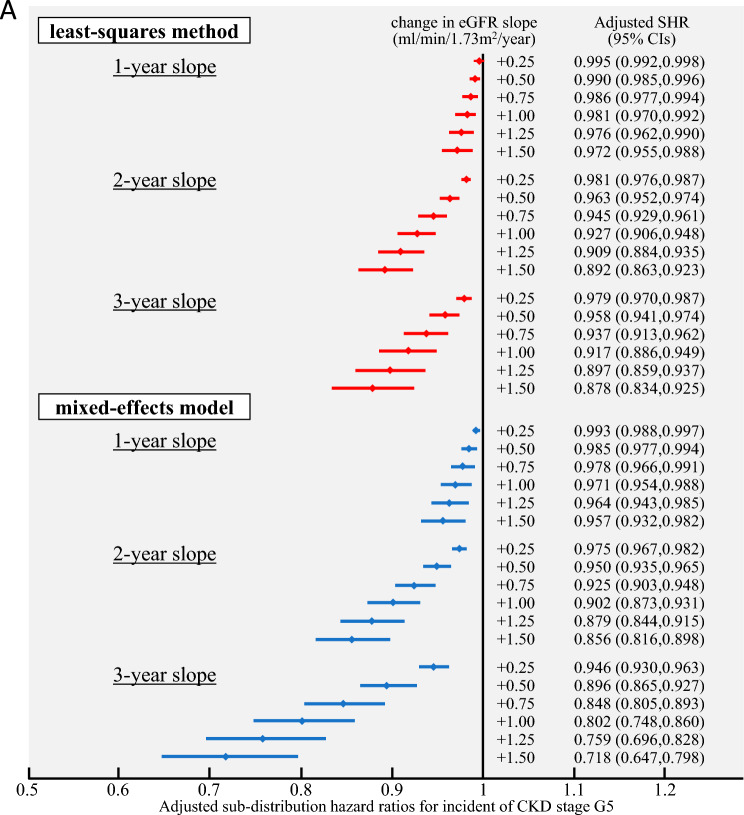
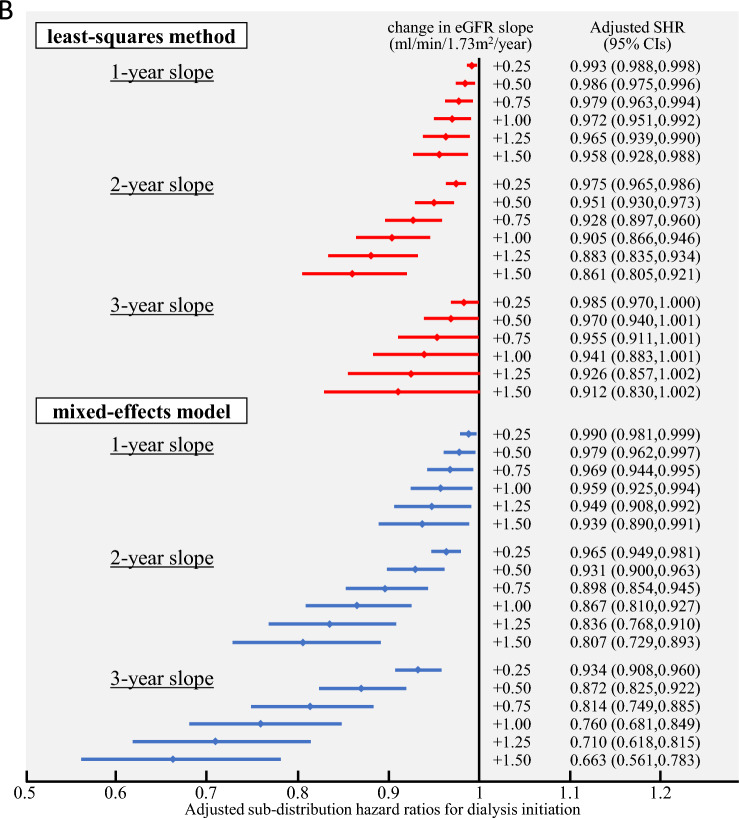
Results: Our analysis showed an association between eGFR slope and the risk of end-stage kidney disease. A 30% decrease in albuminuria/proteinuria over 2 years corresponded to a 20% decrease in the risk of end-stage kidney disease patients with baseline UACR ≥ 30 mg/gCre or UPCR ≥ 0.15 g/gCre in the analysis of CKD-JAC, though this analysis was not performed on the other database/cohort. Those results suggested similar trends to those of the systematic review.
Conclusion: The results suggested that eGFR slope and decreased albuminuria/proteinuria may be used as a surrogate endpoint in clinical trials for early CKD (including diabetic kidney disease) in Japanese population, though its validity and cutoff values must be carefully considered based on the latest evidence and other factors.
Keywords: Albuminuria; Chronic kidney disease; Diabetic kidney disease; Proteinuria; Surrogate endpoint; eGFR slope.
© 2024. The Author(s).
Conflict of interest statement
All members involved in creating the guidelines submitted conflict of interest statements based on the rules of the academic society. The specific conflict of interest statements are as follows: Employment: Wataru Asakura, Office of New Drug I, Pharmaceuticals and Medical Devices Agency (PMDA), Tokyo, Japan; Yoshitaka Isaka, Department of Nephrology, Osaka University Graduate School of Medicine, Osaka, Japan; Kunitoshi Iseki, Clinical Research Support Center, Tomishiro Central Hospital, Okinawa, Japan; Kohjiro Ueki, Diabetes Research Center, National Center for Global Health and Medicine, Tokyo, Japan; Tomoko Usui, Division of Nephrology and Endocrinology, Graduate School of Medicine, the University of Tokyo, Tokyo, Japan; Hirokazu Okada, Department of Nephrology, Saitama Medical University, Saitama, Japan; Naoki Kashihara, Department of Nephrology and Hypertension, Kawasaki Medical School, Okayama, Japan; Eiichiro Kanda, Medical Science, Kawasaki Medical School, Okayama, Japan; Masaomi Nangaku, Division of Nephrology and Endocrinology, Graduate School of Medicine, the University of Tokyo, Tokyo, Japan; Kunihiro Matsushita, Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Maryland, USA; Hirotaka Watada, Department of Metabolism and Endocrinology, Juntendo University Graduate School of Medicine, Tokyo, Japan. Consultancies: All the authors, None. Honoraria: Wataru Asakura, Yoshitaka Isaka, Kunitoshi Iseki, Seiji Itano, Tomoko Usui, Eiichiro Kanda, Yuka Sugawara, Mototsugu Tanaka, Koji Tomori, Kunihiro Matsushita, and Yusuke Watanabe, None. Kohjiro Ueki, Sumitomo Pharma Co., Ltd., Novo Nordisk Pharma Ltd., Takeda Pharmaceutical Co., Ltd., Taisho Pharmaceutical Co., Ltd., Eli Lilly Japan K.K., Abbott Japan LLC, Bayer Yakuhin, Ltd, Kowa Company, Ltd, Nippon Boehringer Ingelheim Co., Ltd., Daiichi Sankyo Ltd.; Hirokazu Okada, Daiichi Sankyo Ltd., AstraZeneca K.K., Mitsubishi Tanabe Pharma Corporation, ONO PHARMACEUTICAL CO., LTD., Nippon Boehringer Ingelheim Co., Ltd., Astellas Pharma Inc., Kyowa Kirin Co., Ltd., Bayer Yakuhin, Ltd, Torii Pharmaceutical Co.,Ltd; Naoki Kashihara, Daiichi Sankyo Ltd., AstraZeneca K.K., Mitsubishi Tanabe Pharma Corporation, ONO PHARMACEUTICAL CO., LTD., Nippon Boehringer Ingelheim Co., Ltd., Astellas Pharma Inc., Kyowa Kirin Co., Ltd., Bayer Yakuhin, Ltd, Nobelpharma Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Novartis Pharma K.K., Yusuke Suzuki, Kyowa Kirin Co., Ltd., Mitsubishi Tanabe Pharma Corporation, Novartis Pharma K.K., Daiichi Sankyo Ltd., Otsuka Pharmaceutical Co., Ltd., Otsuka America Pharmaceutical, Inc.; Masaomi Nangaku, Kyowa Kirin Co., Ltd., Astellas Pharma Inc., Mitsubishi Tanabe Pharma Corporation, Bayer Yakuhin, Ltd, Japan Tobacco Inc.; Rimei Nishimura, Eli Lilly Japan K.K., Kissei Pharmaceutical Co., Ltd., Novo Nordisk Pharma Ltd., MEDTRONIC JAPAN CO., LTD., ONO PHARMACEUTICAL CO., LTD., Mitsubishi Tanabe Pharma Corporation, Sanofi K.K., Nippon Boehringer Ingelheim Co., Ltd., Astellas Pharma Inc., Abbott Japan LLC; Takayuki Hamano, Astellas Pharma Inc., Torii Pharmaceutical Co.,Ltd., Kyowa Kirin Co., Ltd., Mitsubishi Tanabe Pharma Corporation, Chugai Pharmaceutical Co., Ltd., Kissei Pharmaceutical Co., Ltd., Sanwa Kagaku Kenkyusho Co., Ltd., Otsuka Pharmaceutical Co., Ltd., ONO PHARMACEUTICAL CO., LTD.; Kei Fukami, AstraZeneca K.K., Otsuka Pharmaceutical Co., Ltd., Nobelpharma Co., Ltd., ONO PHARMACEUTICAL CO., LTD., Bayer Yakuhin, Ltd, Kyowa Kirin Co., Ltd., Nippon Boehringer Ingelheim Co., Ltd., Sumitomo Pharma Co., Ltd., Mitsubishi Tanabe Pharma Corporation; Jun Wada, AstraZeneca K.K., Mitsubishi Tanabe Pharma Corporation; Hirotaka Watada, Mitsubishi Tanabe Pharma Corporation, Taisho Pharmaceutical Co., Ltd., Novo Nordisk Pharma Ltd., Astellas Pharma Inc., Abbott Japan LLC, MSD K.K., Kissei Pharmaceutical Co., Ltd., AstraZeneca K.K., ONO PHARMACEUTICAL CO., LTD., Sanofi K.K, Sumitomo Pharma Co., Ltd, Eli Lilly Japan K.K., Nippon Boehringer Ingelheim Co., Ltd., Sanwa Kagaku Kenkyusho Co., Ltd., Takeda Pharmaceutical Co., Ltd., Kowa Company, Ltd, Kyowa Kirin Co., Ltd., Terumo Corporation. Stock ownership or options: All the authors, None. Grants received: Wataru Asakura, Yoshitaka Isaka, Kunitoshi Iseki, Seiji Itano, Tomoko Usui, Eiichiro Kanda, Yuka Sugawara, Mototsugu Tanaka, Koji Tomori, Rimei Nishimura, Kei Fukami, Jun Wada, and Yusuke Watanabe, None. Kohjiro Ueki, Nippon Boehringer Ingelheim Co., Ltd., Sumitomo Pharma Co., Ltd, Eli Lilly Japan K.K.; Hirokazu Okada, Kyowa Kirin Co., Ltd., Torii Pharmaceutical Co.,Ltd, Kissei Pharmaceutical Co., Ltd.; Naoki Kashihara, AstraZeneca K.K., Nobelpharma Co., Ltd., Daiichi Sankyo Ltd., Bayer Yakuhin, Ltd.; Yusuke Suzuki, Travere Therapeutics, Inc., Chinook Therapeutics U.S., Inc., Moderna TX, ARGENX IIP BV, Aurinia Pharmaceuticals Inc., Kyowa Kirin Co., Ltd.; Masaomi Nangaku, EPS Corporation, Parexel International Inc., Japan Tobacco Inc.; Takayuki Hamano, Astellas Pharma Inc., Torii Pharmaceutical Co.,Ltd.; Kunitoshi Matsushita, Kyowa Kirin Co., Ltd., Akebia, Kowa Company; Hirotaka Watada, Sanofi K.K., Kowa Company, Ltd, Nippon Boehringer Ingelheim Co., Ltd., Mitsubishi Tanabe Pharma Corporation, ONO PHARMACEUTICAL CO., LTD., MSD K.K., Sanwa Kagaku Kenkyusho Co., Ltd., Sumitomo Pharma Co., Ltd, Taisho Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd., Soiken Holdings Inc.
Figures
Similar articles
-
Change in Albuminuria and GFR as End Points for Clinical Trials in Early Stages of CKD: A Scientific Workshop Sponsored by the National Kidney Foundation in Collaboration With the US Food and Drug Administration and European Medicines Agency.Am J Kidney Dis. 2020 Jan;75(1):84-104. doi: 10.1053/j.ajkd.2019.06.009. Epub 2019 Aug 28. Am J Kidney Dis. 2020. PMID: 31473020
-
eGFR slope as a surrogate endpoint for end-stage kidney disease in patients with diabetes and eGFR > 30 mL/min/1.73 m2 in the J-DREAMS cohort.Clin Exp Nephrol. 2024 Feb;28(2):144-152. doi: 10.1007/s10157-023-02408-z. Epub 2023 Oct 9. Clin Exp Nephrol. 2024. PMID: 37806976 Free PMC article.
-
Risk of Progression of Nonalbuminuric CKD to End-Stage Kidney Disease in People With Diabetes: The CRIC (Chronic Renal Insufficiency Cohort) Study.Am J Kidney Dis. 2018 Nov;72(5):653-661. doi: 10.1053/j.ajkd.2018.02.364. Epub 2018 May 18. Am J Kidney Dis. 2018. PMID: 29784612
-
The Validity of Drug Effects on Proteinuria, Albuminuria, Serum Creatinine, and Estimated GFR as Surrogate End Points for ESKD: A Systematic Review.Am J Kidney Dis. 2018 Dec;72(6):779-789. doi: 10.1053/j.ajkd.2018.06.011. Epub 2018 Aug 24. Am J Kidney Dis. 2018. PMID: 30149958
-
Change in albuminuria as a surrogate endpoint.Curr Opin Nephrol Hypertens. 2019 Nov;28(6):519-526. doi: 10.1097/MNH.0000000000000541. Curr Opin Nephrol Hypertens. 2019. PMID: 31449083 Review.
Cited by
-
Shared Decision-Making in Choosing Dialysis Modalities for Patients With Chronic Kidney Disease: An Evolutionary Concept Analysis.Nurs Health Sci. 2025 Jun;27(2):e70099. doi: 10.1111/nhs.70099. Nurs Health Sci. 2025. PMID: 40228796 Free PMC article. Review.
References
-
- Levey AS, Gansevoort RT, Coresh J, Inker LA, Heerspink HL, Grams ME, et al. Change in albuminuria and GFR as end points for clinical trials in early stages of CKD: a scientific workshop sponsored by the National Kidney Foundation in collaboration with the US Food and Drug Administration and European Medicines Agency. Am J Kidney Dis. 2020;75:84–104. 10.1053/j.ajkd.2019.06.009 - DOI - PubMed
-
- Coresh J, Heerspink HJL, Sang Y, Matsushita K, Arnlov J, Astor BC, et al. Change in albuminuria and subsequent risk of end-stage kidney disease: an individual participant-level consortium meta-analysis of observational studies. Lancet Diabetes Endocrinol. 2019;7:115–27. 10.1016/S2213-8587(18)30313-9 - DOI - PMC - PubMed
-
- Grams ME, Sang Y, Ballew SH, Matsushita K, Astor BC, Carrero JJ, et al. Evaluating glomerular filtration rate slope as a surrogate end point for ESKD in clinical trials: an individual participant meta-analysis of observational data. J Am Soc Nephrol. 2019;30:1746–55. 10.1681/ASN.2019010008 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
