

Cost-effectiveness of single-pill and separate-pill administration of antihypertensive triple combination therapy: a population-based microsimulation study
- PMID: 38971775
- PMCID: PMC11227134
- DOI: 10.1186/s12889-024-19346-4
Cost-effectiveness of single-pill and separate-pill administration of antihypertensive triple combination therapy: a population-based microsimulation study
Abstract
Background: Single-pill combination (SPC) of three antihypertensive drugs has been shown to improve adherence to therapy compared with free combinations, but little is known about its long-term costs and health consequences. This study aimed to evaluate the lifetime cost-effectiveness profile of a three-drug SPC of an angiotensin-converting enzyme inhibitor, a calcium-channel blocker, and a diuretic vs the corresponding two-pill administration (a two-drug SPC plus a third drug separately) from the Italian payer perspective.
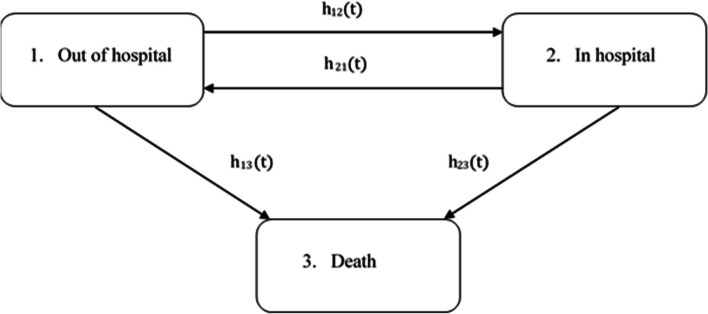
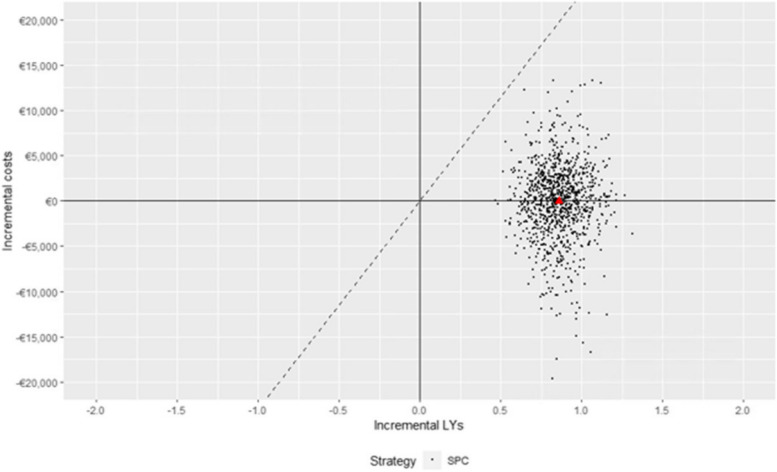
Methods: A cost-effectiveness analysis was conducted using multi-state semi-Markov modeling and microsimulation. Using the healthcare utilization database of the Lombardy Region (Italy), 30,172 and 65,817 patients aged ≥ 40 years who initiated SPC and two-pill combination, respectively, between 2015 and 2018 were identified. The observation period extended from the date of the first drug dispensation until death, emigration, or December 31, 2019. Disease and cost models were parametrized using the study cohort, and a lifetime microsimulation was applied to project costs and life expectancy for the compared strategies, assigning each of them to each cohort member. Costs and life-years gained were discounted by 3%. Probabilistic sensitivity analysis with 1,000 samples was performed to address parameter uncertainty.
Results: Compared with the two-pill combination, the SPC increased life expectancy by 0.86 years (95% confidence interval [CI] 0.61-1.14), with a mean cost differential of -€12 (95% CI -9,719-8,131), making it the dominant strategy (ICER = -14, 95% CI -€15,871-€7,113). The cost reduction associated with the SPC was primarily driven by savings in hospitalization costs, amounting to €1,850 (95% CI 17-7,813) and €2,027 (95% CI 19-8,603) for patients treated with the SPC and two-pill combination, respectively. Conversely, drug costs were higher for the SPC (€3,848, 95% CI 574-10,640 vs. €3,710, 95% CI 263-11,955). The cost-effectiveness profile did not significantly change according to age, sex, and clinical status.
Conclusions: The SPC was projected to be cost-effective compared with the two-pill combination at almost all reasonable willingness-to-pay thresholds. As it is currently prescribed to only a few patients, the widespread use of this strategy could result in benefits for both patients and the healthcare system.
Keywords: Cost-effectiveness; Healthcare utilization database; Hypertension; Microsimulation; Real world; Single-pill combination.
© 2024. The Author(s).
Conflict of interest statement
GC received research support from the European Community (EC), the Italian Agency of Drug (AIFA), and the Italian Ministry of Education, University and Research (MIUR). He took part to a variety of projects that were funded by pharmaceutical companies (i.e., Novartis, GSK, Roche, AMGEN, BMS and Servier). He also received honoraria as member of Advisory Board from Roche. GM2 received honoraria for participation as speaker/chairman in national/international meetings from Bayer, Boehringer Ingelheim, CVRx, Daiichi Sankyo, Ferrer, Medtronic, Menarini Int., Merck, Novartis, Recordati and Servier.
Other authors declare that they have no competing interests.
Figures
References
-
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from. to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 1990, 2021(398), pp. 957–80.1. [1] NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 1990;2021(398):957–80. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
