

Hypothyroidism after hemithyroidectomy: a systematic review and meta-analysis
- PMID: 38972987
- PMCID: PMC11229296
- DOI: 10.1186/s13044-024-00200-z
Hypothyroidism after hemithyroidectomy: a systematic review and meta-analysis
Abstract
Background: The incidence of hypothyroidism following hemithyroidectomy and risk factors associated with its occurrence are not completely understood. This systematic review investigated the incidence and risk factors for hypothyroidism, thyroxine supplementation following hemithyroidectomy as well as the course of post-operative hypothyroidism, including the time to hypothyroidism and incidence of transient hypothyroidism.
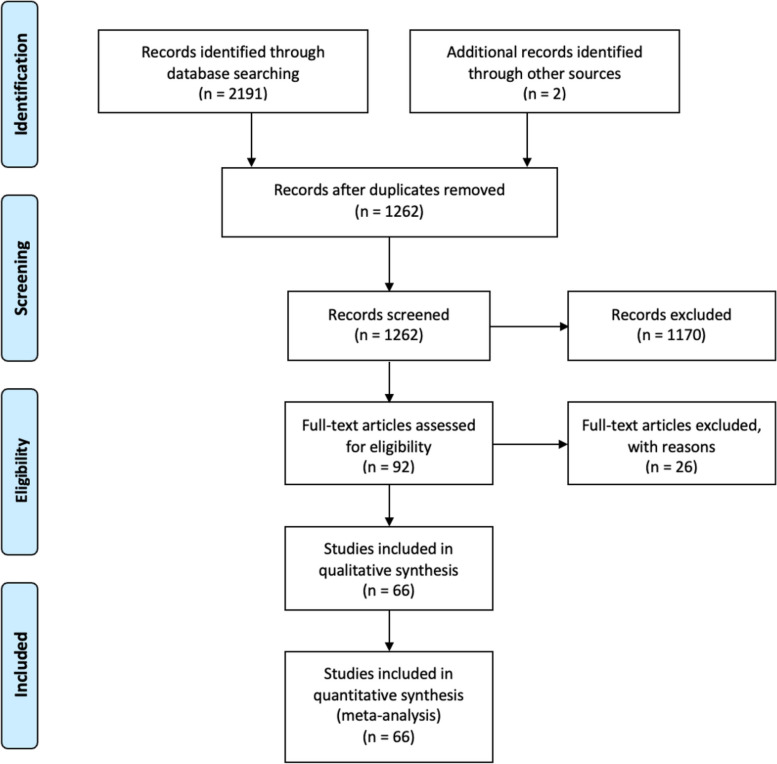
Methods: Searches were conducted in MEDLINE, EMBASE, Scopus, and Cochrane library for studies reporting the incidence of hypothyroidism or thyroxine supplementation following hemithyroidectomy.
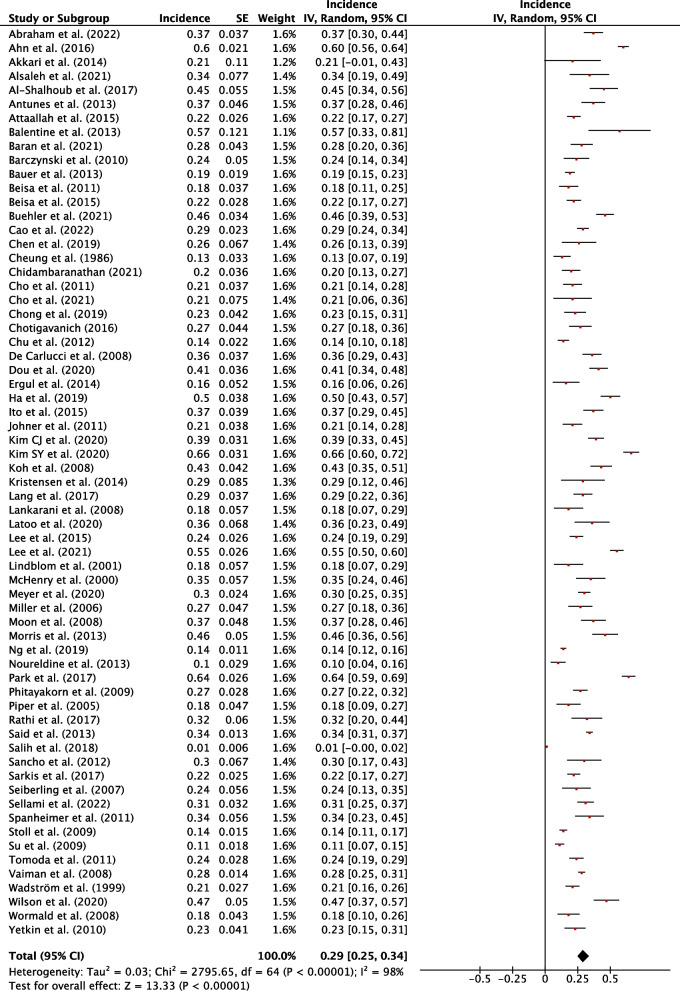
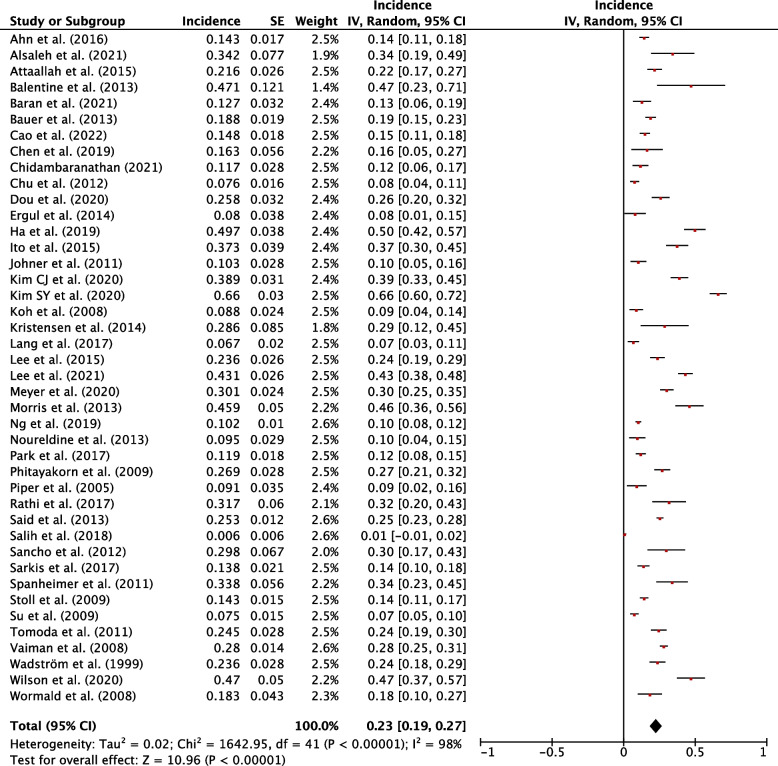
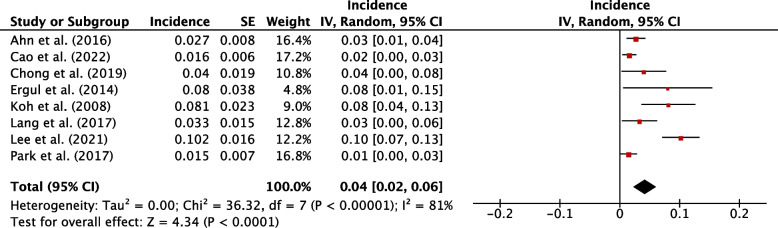
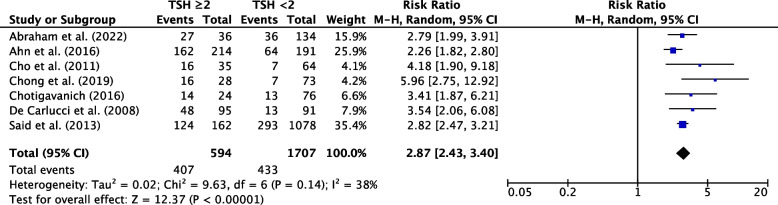
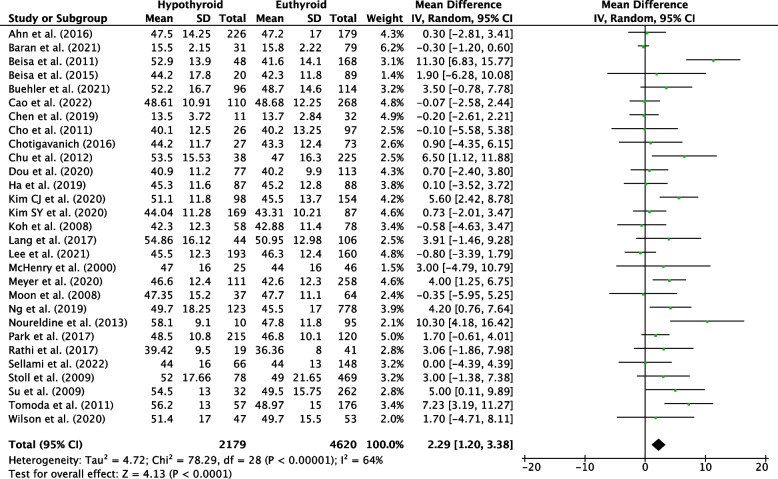
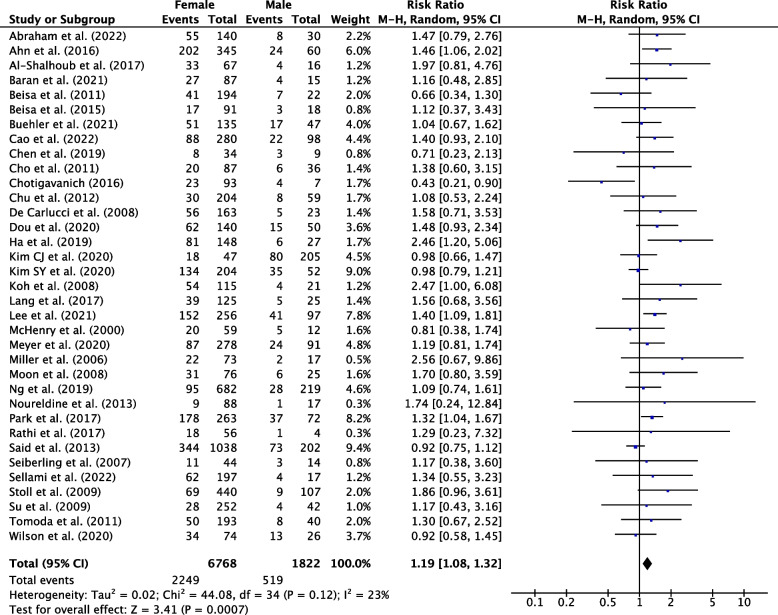
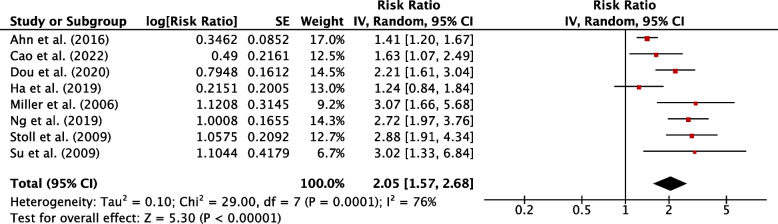
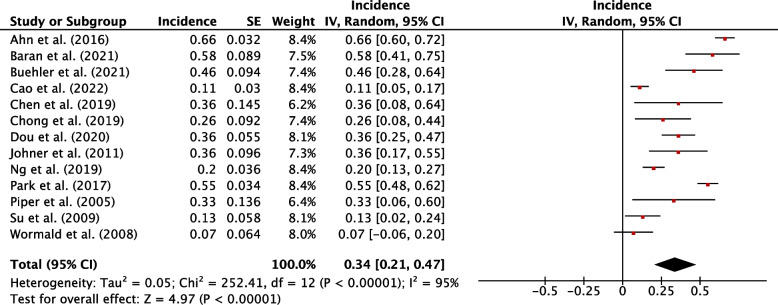
Results: Sixty-six studies were eligible for inclusion: 36 reported risk factors, and 27 reported post-operative course of hypothyroidism. Median follow-up was 25.2 months. The pooled incidence of hypothyroidism was 29% (95% CI, 25-34%; P<0.001). Transient hypothyroidism occurred in 34% of patients (95% CI, 21-47%; P<0.001). The pooled incidence of thyroxine supplementation was 23% (95% CI, 19-27%; P<0.001), overt hypothyroidism 4% (95% CI, 2-6%, P<0.001). Risk factors for development of hypothyroidism included pre-operative thyroid stimulating hormone (TSH) (WMD, 0.87; 95% CI, 0.75-0.98; P<0.001), TSH ≥ 2 mIU/L (RR, 2.87; 95% CI, 2.43-3.40; P<0.001), female sex (RR, 1.19; 95% CI, 1.08-1.32; P=0.007), age (WMD, 2.29; 95% CI, 1.20-3.38; P<0.001), right sided hemithyroidectomy (RR, 1.35; 95% CI, 1.10-1.65, P=0.003), the presence of autoantibodies anti-TPO (RR, 1.92; 95% CI, 1.49-2.48; P<0.001), anti-Tg (RR, 1.53; 95% CI, 1.40-1.88; P<0.001), and Hashimoto's thyroiditis (RR, 2.05; 95% CI, 1.57-2.68; P=0.001).
Conclusion: A significant number of patients will develop hypothyroidism or require thyroxine following hemithyroidectomy. An awareness of patient risk factors and postoperative thyroid function course will assist in counselling patients on their risk profile and guiding management.
Keywords: Hemithyroidectomy; Hypothyroid; Hypothyroidism; Thyroid lobectomy; Thyroxine.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Levothyroxine Supplementation Following Hemithyroidectomy: Incidence, Risk Factors, and Characteristics.Ann Surg Oncol. 2019 Dec;26(13):4405-4413. doi: 10.1245/s10434-019-07786-x. Epub 2019 Sep 5. Ann Surg Oncol. 2019. PMID: 31489555
-
Prevalence of and risk factors for hypothyroidism after hemithyroidectomy: a systematic review and meta-analysis.Endocrine. 2020 Nov;70(2):243-255. doi: 10.1007/s12020-020-02410-5. Epub 2020 Jul 7. Endocrine. 2020. PMID: 32638212
-
Posthemithyroidectomy Hypothyroidism: Updated Meta-Analysis of Risk Factors and Rates of Remission.J Surg Res. 2024 Jan;293:102-120. doi: 10.1016/j.jss.2023.08.020. Epub 2023 Sep 19. J Surg Res. 2024. PMID: 37734294
-
Development of a predictive score for post-hemithyroidectomy hypothyroidism using skeletal muscle index, remnant thyroid index, and thyroid-stimulating hormone levels: a retrospective cohort study.Quant Imaging Med Surg. 2023 Sep 1;13(9):5525-5535. doi: 10.21037/qims-23-53. Epub 2023 Jul 7. Quant Imaging Med Surg. 2023. PMID: 37711833 Free PMC article.
-
Effect of levothyroxine supplementation on pregnancy loss and preterm birth in women with subclinical hypothyroidism and thyroid autoimmunity: a systematic review and meta-analysis.Hum Reprod Update. 2019 May 1;25(3):344-361. doi: 10.1093/humupd/dmz003. Hum Reprod Update. 2019. PMID: 30951172
Cited by
-
Changes in thyroid function after thermal ablation of thyroid nodules.Front Endocrinol (Lausanne). 2025 Feb 27;16:1557725. doi: 10.3389/fendo.2025.1557725. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40084143 Free PMC article.
-
Incidence and risk factors for early thyroxin supplementation therapy after hemithyroidectomy for benign conditions in Europe. A Eurocrine® registry-based study.Updates Surg. 2025 Apr 29. doi: 10.1007/s13304-025-02220-2. Online ahead of print. Updates Surg. 2025. PMID: 40299232
-
Italian guidelines for the management of adult individuals with primary hypothyroidism outside pregnancy.J Endocrinol Invest. 2025 Jul 23. doi: 10.1007/s40618-025-02652-y. Online ahead of print. J Endocrinol Invest. 2025. PMID: 40699541
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
