

Clinical impact of EGFR and KRAS mutations in surgically treated unifocal and multifocal lung adenocarcinoma
- PMID: 38973951
- PMCID: PMC11225054
- DOI: 10.21037/tlcr-24-165
Clinical impact of EGFR and KRAS mutations in surgically treated unifocal and multifocal lung adenocarcinoma
Abstract
Background: Epidermal growth factor receptor (EGFR) and Kirsten rat sarcoma (KRAS) are the two most common oncogenic drivers in lung adenocarcinoma, and their roles still need further exploration. Here we aimed to compare the clinical impact of EGFR and KRAS mutations on disease progression in resected unifocal and multifocal lung adenocarcinoma.
Methods: Clinicopathologic and genomic data were collected for patients who underwent resection of lung adenocarcinoma from 2008 to 2022 at Stanford University Hospital. Retrospective review was performed in 241 patients whose tumors harbored EGFR (n=150, 62.2%) or KRAS (n=91, 37.8%) mutations. Clinical outcome was analyzed with special attention to the natural history of secondary nodules in multifocal cases wherein the dominant tumor had been resected.
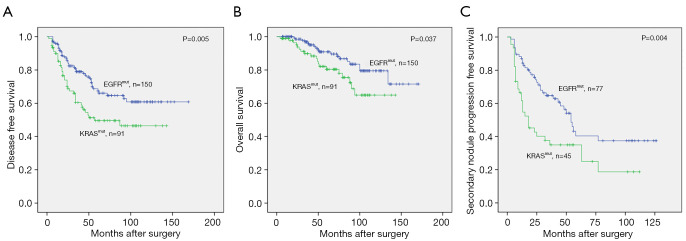
Results: We confirm that compared with EGFR mutations, patients with KRAS mutations had more smokers, larger tumor size, higher TNM stage, higher positron emission tomography (PET)/computed tomography (CT) standard uptake value max, higher tumor mutation burden, and worse disease-free survival and overall survival on univariate analysis. For patients with multifocal pulmonary nodules, the median follow-up of unresected secondary nodules was 55 months. Secondary nodule progression-free survival (SNPFS) was significantly worse for patients with KRAS mutations than those with EGFR mutations (mean 40.3±6.6 vs. 67.7±6.5 months, P=0.004). Univariate analysis showed tumor size, tumor morphology, pathologic TNM stage, and KRAS mutations were significantly associated with SNPFS, while multivariate analysis showed only KRAS mutations were independently associated with worse SNPFS (hazard ratio 1.752, 95% confidence interval: 1.017-3.018, P=0.043).
Conclusions: Resected lung adenocarcinomas with KRAS mutations have more aggressive clinicopathological features and confer worse prognosis than those with EGFR mutations. Secondary pulmonary nodules in multifocal cases with dominant KRAS-mutant tumors have more rapid progression of the secondary nodules.
Keywords: Epidermal growth factor receptor (EGFR); Kirsten rat sarcoma (KRAS); lung adenocarcinoma; multifocal pulmonary nodules.
2024 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-24-165/coif). N.S.L. received research grants with payments from Intuitive Foundation Centese, consulting fees as data safety monitor for clinical trial with payments from Intuitive Surgical, and honoraria for lecture from MEC MMC; W.L.T. purchased stock in these companies (Eli Lilly and Company, Amgen Inc. Kiniksa Pharmaceuticals) several months ago for reasons unrelated to this manuscript; L.M.B. received Research Grant from Department of Veterans Affairs, Chan Zuckerberg Foundation and NIH, and received speaker bureaus/honoraria from MJH Health Sciences, and from Kazan LLP and Craddick LLP for legal expert consulting, and served on Advisory Board for Genentech, Bristol Meyers Squibb, Astra Zeneca and Ethicon/Johnson& Johnson, and served as Board of Directors from Society of Thoracic Surgeons; J.B.S. received payment of consulting on immunotherapy for lung cancer from Astra Zeneca, and was Chair of Society of Thoracic Surgeons Workforce on General Thoracic Surgery (unpaid). The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Dual-energy spectral CT characteristics in surgically resected lung adenocarcinoma: comparison between Kirsten rat sarcoma viral oncogene mutations and epidermal growth factor receptor mutations.Cancer Imaging. 2019 Nov 29;19(1):77. doi: 10.1186/s40644-019-0261-1. Cancer Imaging. 2019. PMID: 31783917 Free PMC article.
-
Kirsten Rat Sarcoma Virus Mutations Effect On Tumor Doubling Time And Prognosis Of Solid Dominant Stage I Lung Adenocarcinoma.Clin Lung Cancer. 2025 May;26(3):210-220.e1. doi: 10.1016/j.cllc.2025.01.001. Epub 2025 Jan 9. Clin Lung Cancer. 2025. PMID: 39863430
-
The prognostic value of Kirsten rat sarcoma viral oncogene homolog mutations in resected lung adenocarcinoma differs according to clinical features.J Thorac Cardiovasc Surg. 2022 Jan;163(1):e73-e85. doi: 10.1016/j.jtcvs.2020.05.097. Epub 2020 Jun 21. J Thorac Cardiovasc Surg. 2022. PMID: 32739163
-
Concordant and Discordant EGFR Mutations in Patients With Multifocal Adenocarcinomas: Implications for EGFR-Targeted Therapy.Clin Ther. 2016 Jul;38(7):1567-76. doi: 10.1016/j.clinthera.2016.06.005. Epub 2016 Jun 29. Clin Ther. 2016. PMID: 27368115 Free PMC article. Review.
-
KRAS mutations in lung cancer.Clin Lung Cancer. 2013 May;14(3):205-14. doi: 10.1016/j.cllc.2012.09.007. Epub 2012 Nov 1. Clin Lung Cancer. 2013. PMID: 23122493 Review.
Cited by
-
Pan-cancer analysis to character the clinicopathological and genomic features of KRAS-mutated patients in China.J Cancer Res Clin Oncol. 2025 Feb 27;151(2):94. doi: 10.1007/s00432-025-06118-9. J Cancer Res Clin Oncol. 2025. PMID: 40016583 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous