

Comparison of postoperative clinical outcomes and knee stability of cruciate-retaining total knee arthroplasty using the tibia-first gap navigation technique with a computer-aided system and measured-resection technique: A retrospective analysis of a propensity-matched cohort
- PMID: 38974051
- PMCID: PMC11224964
- DOI: 10.1002/jeo2.12084
Comparison of postoperative clinical outcomes and knee stability of cruciate-retaining total knee arthroplasty using the tibia-first gap navigation technique with a computer-aided system and measured-resection technique: A retrospective analysis of a propensity-matched cohort
Abstract
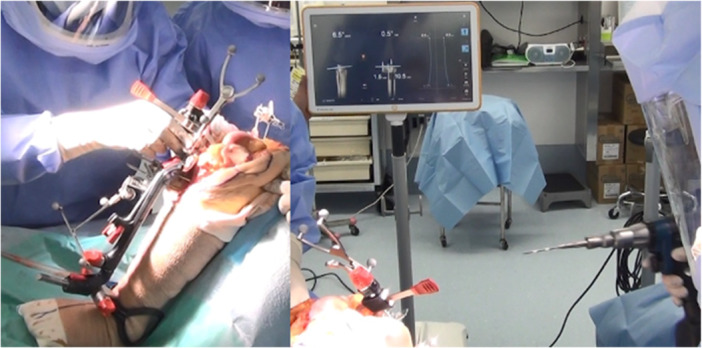
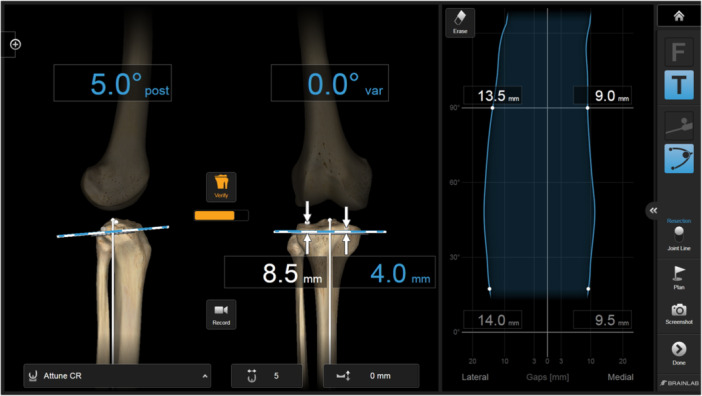
Purpose: This study aimed to clarify whether the range of motion (ROM), anterior and posterior (AP) stability and other clinical measures changed in patients who underwent tibia-first total knee arthroplasty (TF-TKA) using navigation with a computer-aided system after surgery.
Methods: This is a retrospective study and we conducted a matched cohort analysis of 60 measured resection (MR)-TKAs and 52 TF-TKAs performed by a single surgeon. All the surgeries used the same implant and approach. Baseline differences between the groups were adjusted using propensity score matching. We compared each patient's measured ROM and Oxford Knee Score (OKS) and performed knee AP laxity measurements by using a device during routine follow-ups.
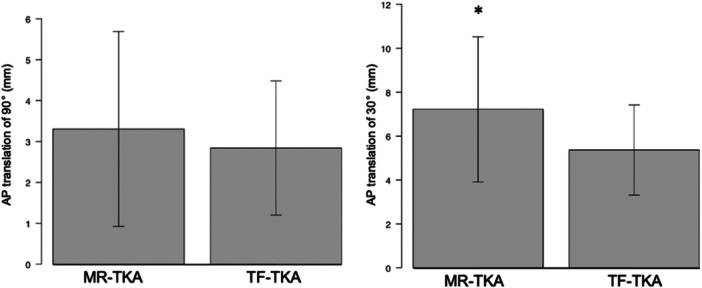
Results: A total of 40 MR-TKAs with a mean age of 73.5 ± 5.6 years and sex (male 10, female 30) were compared to 40 TF-TKAs with a mean age of 74.0 ± 5.7 years and sex (male 13, female 27) at 2-year follow-ups. Two years postoperatively, there was a significant difference in the AP laxity at 30° of knee flexion between both groups (7.0 ± 3.4 mm vs. 5.2 ± 2.3 mm, p < 0.01). In contrast, no differences were found between both groups for knee flexion (120.8 ± 9° vs. 116.7 ± 9.8°, p = 0.07) and OKS score (41.8 ± 6.9 vs. 41.0 ± 5.9, p = 0.61).
Conclusion: The AP stability in the midflexion obtained using the tibia-first technique remained consistent even after 2 years. However, OKS and ROM were not significantly different from those of the MR-TKA group.
Level of evidence: Retrospective comparative LEVEL III study.
Keywords: anterior and posterior knee stability; computer‐assist surgery; tibia‐first technique; total knee osteoarthritis.
© 2024 The Author(s). Journal of Experimental Orthopaedics published by John Wiley & Sons Ltd on behalf of European Society of Sports Traumatology, Knee Surgery and Arthroscopy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Can tibia-first total knee arthroplasty using computer-assisted system improve anterior and posterior knee stability?Technol Health Care. 2022;30(5):1147-1154. doi: 10.3233/THC-213535. Technol Health Care. 2022. PMID: 35599511
-
Comparison of postoperative clinical outcome in medial-pivotal and gradually reducing radius design cruciate-retaining total knee arthroplasty-A multicenter analysis of propensity-matched cohorts.J Exp Orthop. 2024 Jan 19;11(1):e12002. doi: 10.1002/jeo2.12002. eCollection 2024 Jan. J Exp Orthop. 2024. PMID: 38455450 Free PMC article.
-
CR-lipped bearing is an adequate functional solution to patients with perioperative excessive laxity in cruciate retaining total knee arthroplasty.Knee. 2021 Jan;28:51-56. doi: 10.1016/j.knee.2020.11.004. Epub 2020 Dec 8. Knee. 2021. PMID: 33307319
-
Anteroposterior translation and range of motion after total knee arthroplasty using posterior cruciate ligament-retaining versus posterior cruciate ligament-substituting prostheses.Knee Surg Sports Traumatol Arthrosc. 2017 Nov;25(11):3536-3542. doi: 10.1007/s00167-016-4257-0. Epub 2016 Aug 2. Knee Surg Sports Traumatol Arthrosc. 2017. PMID: 27485124
-
How does the use of quantified gap-balancing affect component positioning and limb alignment in robotic total knee arthroplasty using functional alignment philosophy? A comparison of two robotic platforms.Int Orthop. 2023 May;47(5):1221-1232. doi: 10.1007/s00264-022-05681-x. Epub 2023 Feb 6. Int Orthop. 2023. PMID: 36740610 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
