

Atypical Presentation of Idiopathic Intracranial Hypertension: A Case Series and Literature Review
- PMID: 38974423
- PMCID: PMC11226282
- DOI: 10.1055/s-0044-1779447
Atypical Presentation of Idiopathic Intracranial Hypertension: A Case Series and Literature Review
Abstract
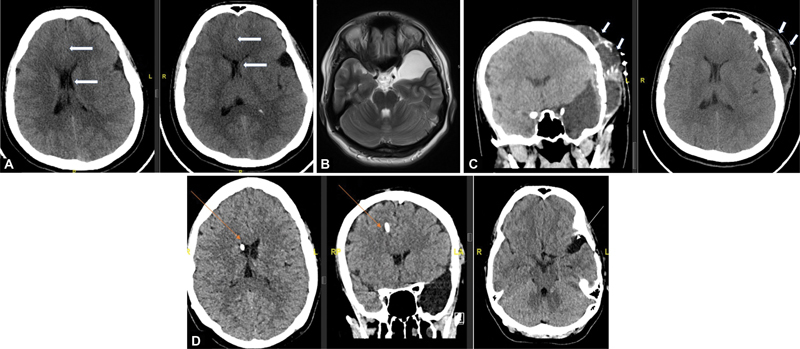
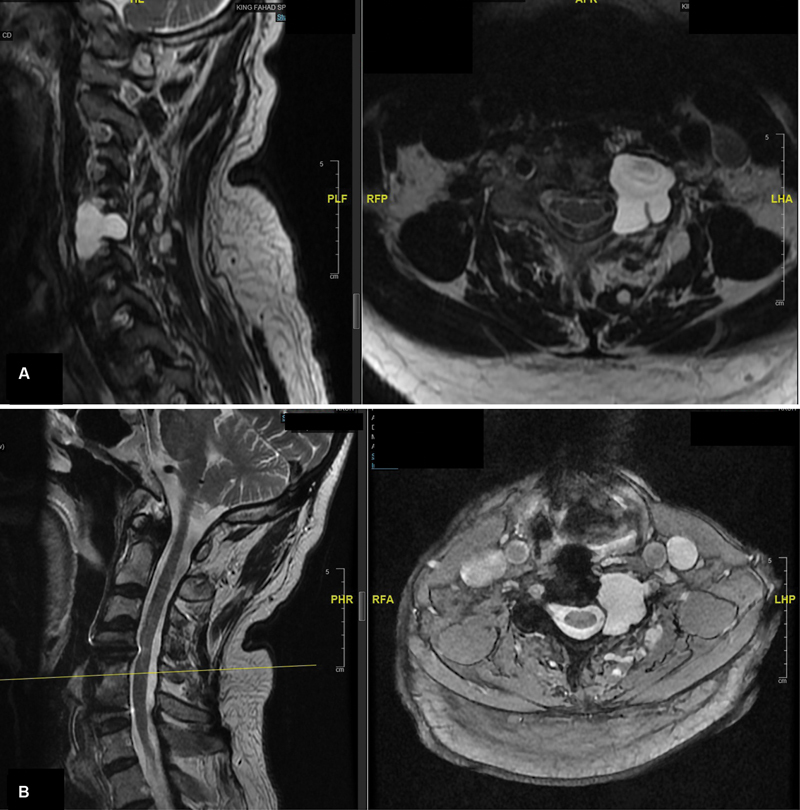
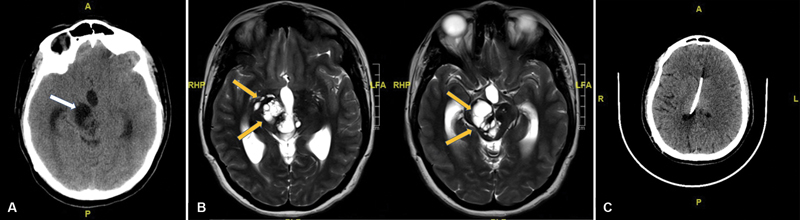
Idiopathic intracranial hypertension (IIH) is a condition in which intracranial pressure (ICP) increases without an apparent cause. Typically, patients present with headaches, dizziness, pulsatile tinnitus, visual disturbances, blurred vision, diplopia, photophobia, visual field defects, and papilledema on fundoscopy. The association between IIH, spontaneous cerebrospinal fluid (CSF) rhinorrhea, and arachnoid cysts has been discussed in the literature; however, there is no clear explanation for this association. We aimed to present a series of four patients with a confirmed diagnosis of IIH with atypical presentations, discuss the management of each case, and provide an explanation for this association to alert clinicians to the atypical presentation of IIH and facilitate early diagnosis and proper treatment of this condition by CSF diversion. This was a retrospective case series of all patients who were diagnosed with IIH and showed improvement after ventriculoperitoneal shunt insertion after failure of at least one operative intervention resulting from primary radiological and clinical findings in 2001 to 2022. Data on demographics, clinical presentation, radiological findings, surgical management, and diagnostic criteria for IIH were recorded. We identified four patients with a confirmed diagnosis of IIH who presented with atypical presentations as follows: intracranial arachnoid cyst, cervical spine arachnoid cyst, giant Virchow perivascular space, and spontaneous CSF (CSF) rhinorrhea. All patients responded to CSF diversion after failure of surgical treatment targeting the primary pathology. IIH should be suspected after the failure of primary surgical treatment in cases of spontaneous CSF rhinorrhea, spinal and cranial arachnoid cysts, and symptomatic ventriculoperitoneal shunt. Treatment in such situations should be directed toward IIH with CSF diversion.
Keywords: Virchow perivascular space; arachnoid cyst; idiopathic intracranial hypertension; lumboperitoneal shunt; spontaneous CSF rhinorrhea.
Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
Spontaneous cerebrospinal fluid rhinorrhea as a primary presentation of idiopathic intracranial hypertension, management strategies, and clinical outcome.Surg Neurol Int. 2024 Dec 11;15:458. doi: 10.25259/SNI_560_2024. eCollection 2024. Surg Neurol Int. 2024. PMID: 39777167 Free PMC article.
-
Primary spontaneous cerebrospinal fluid leaks and idiopathic intracranial hypertension.J Neuroophthalmol. 2013 Dec;33(4):330-7. doi: 10.1097/WNO.0b013e318299c292. J Neuroophthalmol. 2013. PMID: 24042170 Free PMC article. Review.
-
Cerebrospinal fluid hydrodynamics in arachnoid cyst patients with persistent idiopathic intracranial hypertension: A case series and review.Surg Neurol Int. 2020 Aug 8;11:237. doi: 10.25259/SNI_129_2020. eCollection 2020. Surg Neurol Int. 2020. PMID: 32874740 Free PMC article.
-
Unusual association of cervical arachnoid cyst and idiopathic intracranial hypertension.Neurosciences (Riyadh). 2024 Oct;29(4):284-287. doi: 10.17712/nsj.2024.4.20240005. Neurosciences (Riyadh). 2024. PMID: 39379080 Free PMC article.
-
Do Most Patients With a Spontaneous Cerebrospinal Fluid Leak Have Idiopathic Intracranial Hypertension?J Neuroophthalmol. 2019 Dec;39(4):487-495. doi: 10.1097/WNO.0000000000000761. J Neuroophthalmol. 2019. PMID: 30747786 Free PMC article. Review.
References
-
- Durcan F J, Corbett J J, Wall M. The incidence of pseudotumor cerebri. Population studies in Iowa and Louisiana. Arch Neurol. 1988;45(08):875–877. - PubMed
-
- Kesler A, Goldhammer Y, Gadoth N. Do men with pseudomotor cerebri share the same characteristics as women? A retrospective review of 141 cases. J Neuroophthalmol. 2001;21(01):15–17. - PubMed
-
- Giuseffi V, Wall M, Siegel P Z, Rojas P B.Symptoms and disease associations in idiopathic intracranial hypertension (pseudotumor cerebri): a case-control study Neurology 199141(2 ( Pt 1)):239–244. - PubMed
LinkOut - more resources
Full Text Sources