

[EXTUBATION FAILURE IN BURNS: INCIDENCE, RISK FACTORS AND PROGNOSIS]
- PMID: 38974788
- PMCID: PMC11225298
[EXTUBATION FAILURE IN BURNS: INCIDENCE, RISK FACTORS AND PROGNOSIS]
Abstract
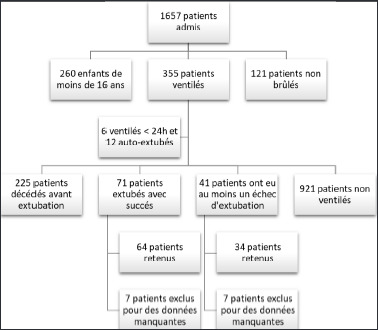
The incidence of extubation failure varies between 2 and 25% depending on the studied population. Few studies have been conducted in burn victims. To determine the incidence, causes, risk factors and outcome of burned patients after a failed extubation, a retrospective single-center case-control study was conducted over a period of 3 years (January 2018-December 2021). All burned patients aged over 16, ventilated for at least 24 hours and having had at least one extubation attempt were included. Extubation failure was defined as the need for re-intubation within 48 hours. Eighty-eight patients had planned extubation. These patients were divided into 2 groups comparable in terms of age and sex. Failure group: including patients with failed extubation (N= 34) and a success group (N= 64) including patients who succeeded. The incidence of extubation failure was 36.6%. Hypophosphatemia, anemia <8g/dl, duration of mechanical ventilation of 8,5 days and abundant secretions during extubation were identified as risk factors for extubation failure (p<0.05). The main cause of failure was retention of secretion (50%). Extubation failure was associated with prolonged length of stay (34 vs. 19 days, P= 0.005), increased infectious complications (P=0.007) and mortality rate (79.4%, 1.5%, P<0.001).
L’échec d’extubation est défini comme la nécessité d’une réintubation dans les 48-72 heures dans les suites d’une extubation programmée. Peu d’études se sont intéressées à ce sujet chez les brûlés. Pour déterminer l’incidence, les causes, les facteurs de risque et l’évolution des patients brûlés ayant subi un échec d’extubation, nous avons conduit une étude monocentrique rétrospective cas - témoin sur une période de 3 ans (janvier 2018 - décembre 2021). Tous les patients brûlés âgés de plus de 16 ans, ventilés pendant au moins 24 heures et ayant eu au moins une tentative d’extubation ont été inclus. Quatre-vingt-dix-huit patients ont eu une extubation programmée. Ces patients ont été répartis en 2 groupes comparables en termes d’âge et de sexe. Groupe «échec» : inclut les patients qui ont échoué l’extubation (N=34), groupe succès : inclut les patients qui l’ont réussie (N=64). L’incidence de l’échec d’extubation était donc de 36,6%. L’hypophosphorémie, l’anémie <8g/dl et les secrétions abondantes en péri - extubation étaient identifiés comme facteurs de risque d’échec d’extubation (p<0,05). Une durée de ventilation mécanique (VM) de 8,5 jours a été identifiée comme prédictive d’échec. La cause principale d’échec d’extubation était la rétention de sécrétions (n=17 : 50%). L’échec d’extubation a été associé à une prolongation de la durée de séjour (34 vs 19 jours, p=0,005), à une augmentation des complications infectieuses (p=0,007) et du taux de mortalité (79,4% vs 1,5%, P< 0,001).
Keywords: burns; extubation; failure; mechanical ventilation; risk factors.
© 2024 Euro-Mediterranean Council for Burns and Fire Disasters.
Figures
Similar articles
-
The incidence and outcome of extubation failure in burn intensive care patients.J Burn Care Res. 2009 May-Jun;30(3):386-92. doi: 10.1097/BCR.0b013e3181a2894c. J Burn Care Res. 2009. PMID: 19349900
-
Extubation Failure in a Burn Intensive Care Unit: Examination of Contributing Factors.J Burn Care Res. 2021 Mar 4;42(2):177-181. doi: 10.1093/jbcr/iraa162. J Burn Care Res. 2021. PMID: 32918478
-
Extubation failure in infants with shunt-dependent pulmonary blood flow and univentricular physiology.Cardiol Young. 2014 Feb;24(1):64-72. doi: 10.1017/S1047951112002181. Epub 2013 Jan 18. Cardiol Young. 2014. PMID: 23328580
-
Extubation failure: magnitude of the problem, impact on outcomes, and prevention.Curr Opin Crit Care. 2003 Feb;9(1):59-66. doi: 10.1097/00075198-200302000-00011. Curr Opin Crit Care. 2003. PMID: 12548031 Review.
-
Decision to extubate.Intensive Care Med. 2002 May;28(5):535-46. doi: 10.1007/s00134-002-1268-8. Epub 2002 Apr 12. Intensive Care Med. 2002. PMID: 12029399 Review.
Cited by
-
The ability of diaphragmatic excursion after extubation to predict the need for resumption of ventilatory support in critically ill surgical patients.J Anesth. 2025 Apr;39(2):189-197. doi: 10.1007/s00540-024-03442-1. Epub 2025 Jan 5. J Anesth. 2025. PMID: 39757317 Free PMC article.
References
-
- Badulak J, Schurr M, Sauaia A, et al. : Defining the criteria for intubation of the patient with thermal burns. Burns, 44: 531-8, 2018. doi: 10.1016/j.burns.2018.02.016 - PubMed
-
- Smailes S, Martin R, McVicar A: The incidence and outcome of extubation failure in burn intensive care patients. J Burn Care Res, 30: 386-92, 2009. doi: 10.1097/BCR.0b013e3181a2894c - PubMed
-
- Blackwood B, Alderdice A, Burns KE, et al. : Protocolized versus non-protocolized weaning for reducing the duration of mechanical ventilation in critically ill adult patients. Cochrane Database Syst Rev, 5: CD006904, 2010. doi: 10.1002/14651858.CD006904.pub2 - PubMed
-
- Boles JM, Bion J, Connors A, et al. : Weaning from mechanical ventilation. Eur Respir J, 29: 1033-56, 2007. doi: 10.1183/09031936.00010206 - PubMed
-
- Rashkin M, Davis T: Acute complications of endotracheal intubation. Relationship to reintubation, route, urgency, and duration. Chest, 89: 165-7, 1986. doi: 10.1378/chest.89.2.165 - PubMed
Publication types
LinkOut - more resources
Full Text Sources