

Differential risks of psoriatic arthritis development in patients with varied psoriasis manifestations: a sex- and ethnicity-specific analysis
- PMID: 38975056
- PMCID: PMC11224429
- DOI: 10.3389/fmed.2024.1385491
Differential risks of psoriatic arthritis development in patients with varied psoriasis manifestations: a sex- and ethnicity-specific analysis
Abstract
Objectives: This study investigated psoriatic arthritis (PsA) risk across varied psoriasis manifestations, considering sex and ethnicity.
Methods: Using TriNetX, a federated database encompassing over 120 million electronic health records (EHRs), we performed global retrospective cohort studies. Psoriasis vulgaris (Pso), pustulosis palmoplantaris (PPP), and generalized pustular psoriasis (GPP) cohorts were retrieved using ICD-10 codes. Propensity score matching, incorporating age, sex, and ethnicity, was employed. An alternative propensity matching model additionally included established PsA risk factors.
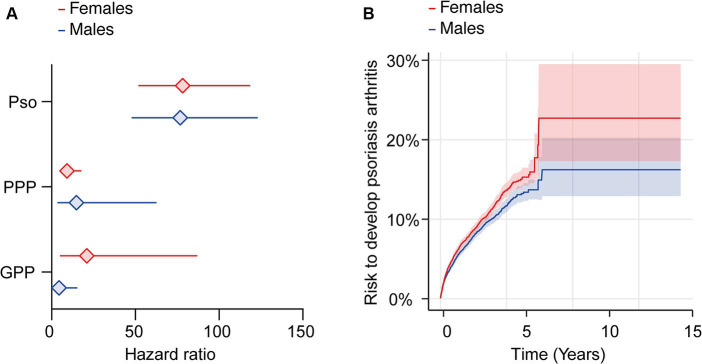
Results: We retrieved data from 486 (Black or African American-stratified, GPP) to 35,281 (Pso) EHRs from the US Collaborative Network. Significant PsA risk variations emerged: Pso carried the highest risk [hazard ratio (HR) 87.7, confidence interval (CI) 63.4-121.1, p < 0.001], followed by GPP (HR 26.8, CI 6.5-110.1, p < 0.0001), and PPP (HR 15.3, CI 7.9-29.5, p < 0.0001). Moreover, we identified significant sex- and ethnicity-specific disparities in PsA development. For instance, compared to male Pso patients, female Pso patients had an elevated PsA risk (HR 1.1, CI 1.1-1.2, p = 0.002). Furthermore, White Pso patients had a higher likelihood of developing PsA compared to their Black or African American counterparts (HR 1.3, CI 1.04-1.7, p = 0.0244). We validated key findings using alternative propensity matching strategies and independent databases.
Conclusion: This study delineates nuanced PsA risk profiles across psoriasis forms, highlighting the pivotal roles of sex and ethnicity. Integrating these factors into PsA risk assessments enables tailored monitoring and interventions, potentially impacting psoriasis patient care quality.
Keywords: TriNetX; arthritis; cohort study; psoriasis; psoriatic arthritis; pustular psoriasis; pustulosis palmoplantaris; risk.
Copyright © 2024 Gershater, Bieber, Vorobyev, Ludwig, Zirpel, De Luca, Thaci, Kridin and Ludwig.
Conflict of interest statement
DT has received honoraria or fees for serving on advisory boards, as a speaker, as a consultant from AbbVie, Amgen, Almirall, Beiersdorf, Bristol-Meiers-Squibb, Boehringer Ingelheim, Galapagos, Leo Pharma, Merck Sharp & Dohme, Morphosys, Lilly, Novartis, Janssen-Cilag, Pfizer, Regeneron, Sanofi, Hexal, Sun Pharmaceuticals, and UCB and grants from Leo Pharma and Novartis. RL has received honoraria for speaking or consulting or has obtained research grants from Monasterium Laboratories, Novartis, Lilly, Bayer, Dompe, Synthon, Argen-X, and Incyte during the last 3 years. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures



Similar articles
-
Interleukin-23 versus Interleukin-17 Inhibitors in Preventing Incidental Psoriatic Arthritis in Patients with Psoriasis: A Real-World Comparison From the TriNetX US Collaborative Network.BioDrugs. 2025 Mar;39(2):297-306. doi: 10.1007/s40259-025-00705-5. Epub 2025 Jan 29. BioDrugs. 2025. PMID: 39875705 Free PMC article.
-
From psoriasis to psoriatic arthritis: epidemiological insights from a retrospective cohort study of 74,046 patients.Front Med (Lausanne). 2024 Jun 27;11:1419722. doi: 10.3389/fmed.2024.1419722. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38994340 Free PMC article.
-
The risk of interstitial lung disease in psoriatic arthritis versus psoriasis: a retrospective nationwide database analysis (2014-24).Rheumatol Adv Pract. 2025 May 27;9(3):rkaf059. doi: 10.1093/rap/rkaf059. eCollection 2025. Rheumatol Adv Pract. 2025. PMID: 40520447 Free PMC article.
-
Systematic review and meta-analysis on prevalence of metabolic syndrome in psoriatic arthritis, rheumatoid arthritis and psoriasis.Int J Rheum Dis. 2021 Sep;24(9):1112-1120. doi: 10.1111/1756-185X.14147. Epub 2021 Jun 2. Int J Rheum Dis. 2021. PMID: 34076348
-
Predictors, Risk Factors, and Incidence Rates of Psoriatic Arthritis Development in Psoriasis Patients: A Systematic Literature Review and Meta-Analysis.Rheumatol Ther. 2021 Dec;8(4):1519-1534. doi: 10.1007/s40744-021-00378-w. Epub 2021 Oct 1. Rheumatol Ther. 2021. PMID: 34596875 Free PMC article. Review.
Cited by
-
A comprehensive review of methodologies and application to use the real-world data and analytics platform TriNetX.Front Pharmacol. 2025 Mar 10;16:1516126. doi: 10.3389/fphar.2025.1516126. eCollection 2025. Front Pharmacol. 2025. PMID: 40129946 Free PMC article. Review.
-
Interleukin-23 versus Interleukin-17 Inhibitors in Preventing Incidental Psoriatic Arthritis in Patients with Psoriasis: A Real-World Comparison From the TriNetX US Collaborative Network.BioDrugs. 2025 Mar;39(2):297-306. doi: 10.1007/s40259-025-00705-5. Epub 2025 Jan 29. BioDrugs. 2025. PMID: 39875705 Free PMC article.
-
Evaluation of the "Multivariable Psoriatic Arthritis Risk Estimation Tool" in a Cohort of Patients with Psoriasis: Preliminary Results of a Prospective Observational Study.Rheumatol Ther. 2025 Feb;12(1):203-209. doi: 10.1007/s40744-024-00729-3. Epub 2024 Dec 5. Rheumatol Ther. 2025. PMID: 39638968 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous