

Effects of pay-for-performance based antimicrobial stewardship on antimicrobial consumption and expenditure: An interrupted time series analysis
- PMID: 38975216
- PMCID: PMC11226823
- DOI: 10.1016/j.heliyon.2024.e32750
Effects of pay-for-performance based antimicrobial stewardship on antimicrobial consumption and expenditure: An interrupted time series analysis
Abstract
Objectives: To evaluate the impact of pay-for-performance on antimicrobial consumption and antimicrobial expenditure in a large teaching hospital in Guangzhou, China.
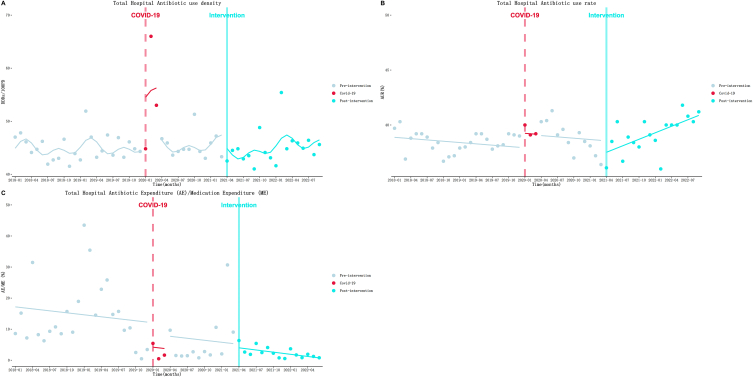
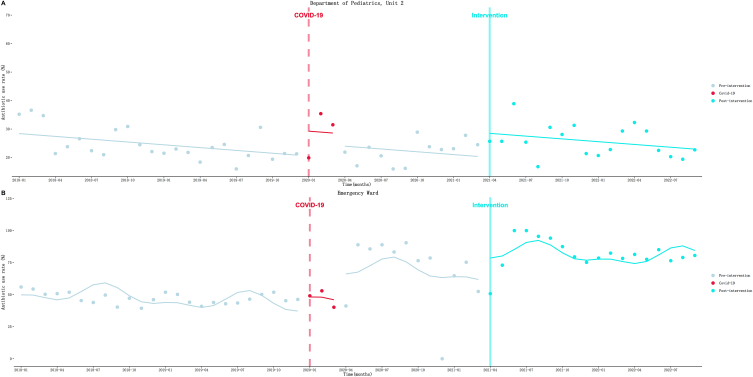
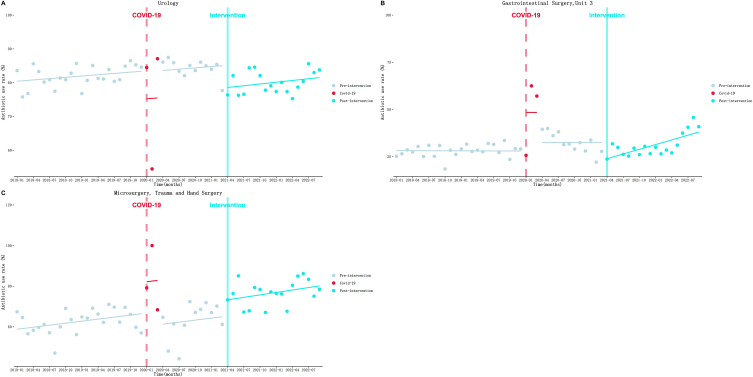
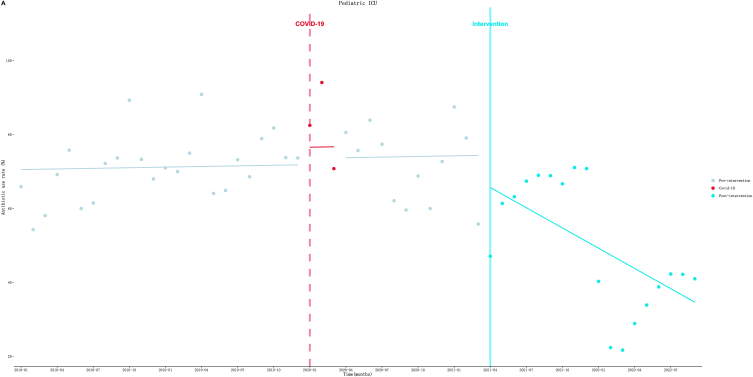
Methods: We collected data from hospital information system from January 2018 through September 2022 in the inpatient wards. Antimicrobial consumption was evaluated using antibiotic use density (AUD) and antibiotic use rate (AUR). The economic impact of intervention was assessed by antimicrobial expenditure percentage. The data was analyzed using interrupted time series (ITS) analysis.
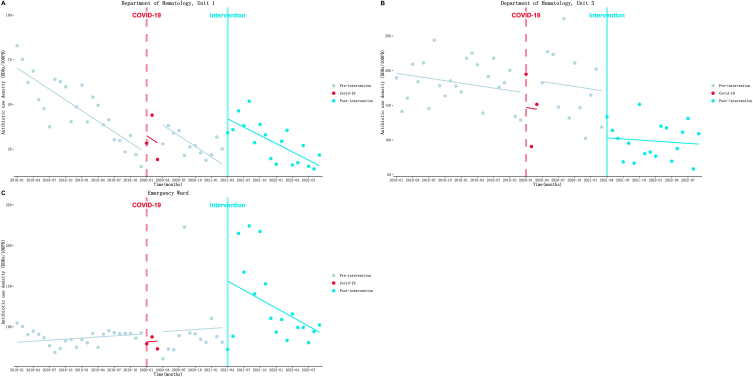
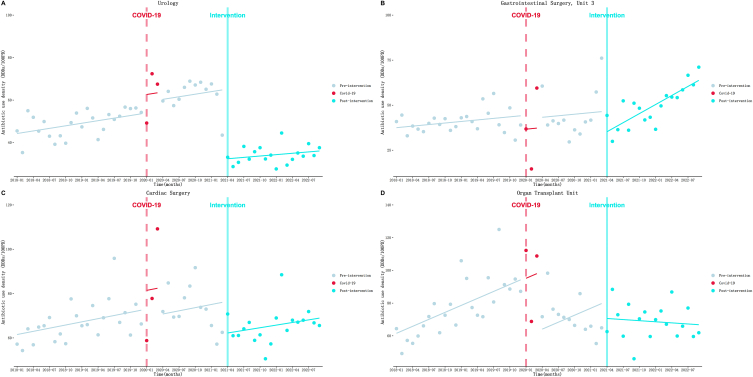
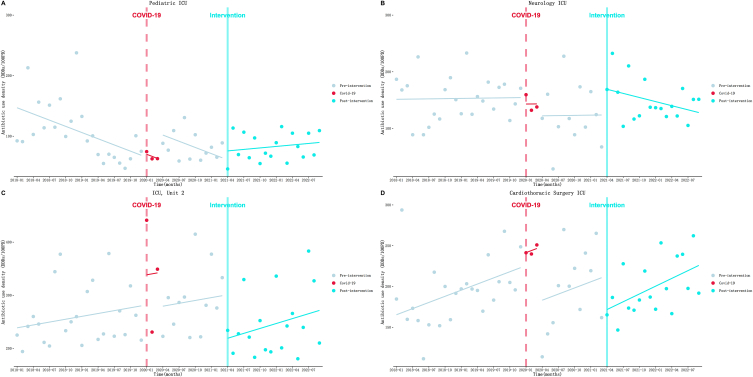
Results: Following the implementation of the intervention, immediate decreases in the level of AUD were observed in Department of Hematology Unit 3 (β = -66.93 DDDs/100PD, P = 0.002), Urology (β = -32.80 DDDs/100PD, P < 0.001), Gastrointestinal Surgery Unit 3 (β = -11.44 DDDs/100PD, P = 0.03), Cardiac Surgery (β = -14.30 DDDs/100PD, P = 0.01), ICU, Unit 2 (β = -81.91 DDDs/100PD, P = 0.02) and Cardiothoracic Surgery ICU (β = -41.52 DDDs/100PD, P = 0.05). Long-term downward trends in AUD were also identified in Organ Transplant Unit (β = -1.64 DDDs/100PD, P = 0.02). However, only Urology (β = -6.56 DDDs/100PD, P = 0.02) and Gastrointestinal Surgery Unit 3 (β = -8.50 %, P = 0.01) showed an immediate decrease in AUR, and long-term downward trends in AUR were observed in Pediatric ICU (β = -1.88 %, P = 0.05) and ICU Unit 1 (β = -0.55 %, P = 0.02).
Conclusion: This study demonstrates that the adoption of pay-for-performance effectively reduces antibiotic consumption in specific departments of a hospital in Guangzhou in the short term. However, it is important to recognize that the long-term impact of such interventions is often limited. Additionally, it should be noted that the overall effectiveness of the intervention across the entire hospital was not significant.
Keywords: Antimicrobial consumption; Antimicrobial stewardship; Interrupted time series analysis; One-off bonus payment; Penalty.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- O’Neill, J. Tackling drug-resistant infections globally: final report and recommendations. (Government of the United Kingdom, May 2016). Available from: https://amr-review.org/sites/default/files/160525_Final%20paper_with%20c..., access on 12 June, 2024.
LinkOut - more resources
Full Text Sources
