

Interferon-α could induce liver steatosis to promote HBsAg loss by increasing triglyceride level
- PMID: 38975233
- PMCID: PMC11226829
- DOI: 10.1016/j.heliyon.2024.e32730
Interferon-α could induce liver steatosis to promote HBsAg loss by increasing triglyceride level
Abstract
Background: The correlation between metabolic syndrome (MetS) and hepatitis B surface antigen (HBsAg) loss remains to be further elucidated, particularly in patients receiving pegylated interferon-α (PEG-IFN) treatment.
Methods: 758 patients with low HBsAg quantification who had received nucleos(t)ide analog (NUC) therapy for at least one year and subsequently switched to or add on PEG-IFN therapy over an unfixed course were enrolled. 412 patients were obtained with baseline data matched. A total of 206 patients achieved HBsAg loss (cured group) within 48 weeks. Demographic and biochemical data associated with MetS were gathered for analysis. HepG2.2.15 cell line was used in vitro experiments to validate the efficacy of interferon-α (IFN-α).
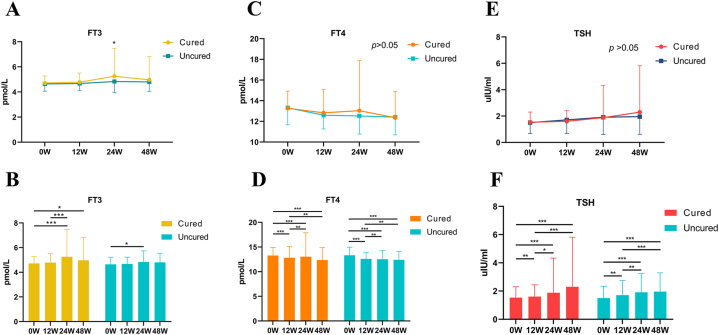
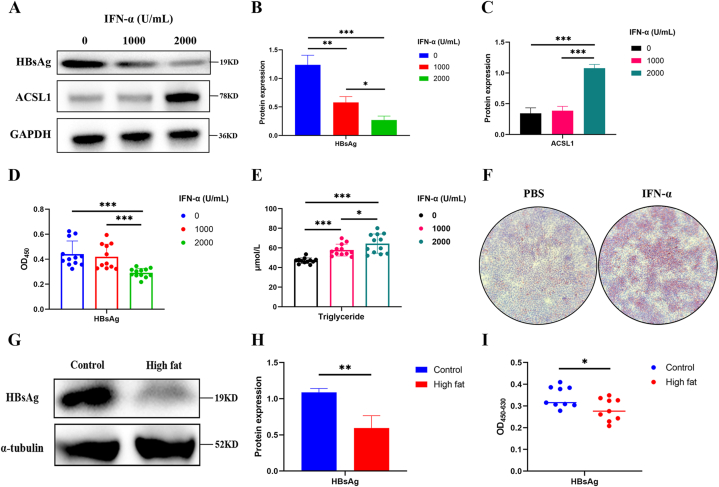
Results: The proportion of patients with diabetes or hypertension in the uncured group was significantly higher than in the cured group. The levels of fasting blood glucose (FBG) and glycated albumin remained elevated in the uncured group over the 48 weeks. In contrast, the levels of blood lipids and uric acid remained higher in the cured group within 48 weeks. Triglycerides levels and liver steatosis of all patients increased after PEG-IFN therapy. Baseline elevated uric acid levels and hepatic steatosis may be beneficial for HBsAg loss. IFN-α could induce hepatic steatosis and indirectly promote HBsAg loss by increasing triglyceride level through upregulation of acyl-CoA synthetase long-chain family member 1(ACSL1).
Conclusions: IFN-α could induce liver steatosis to promote HBsAg loss by increasing triglyceride level through upregulation of ACSL1. Comorbid diabetes may be detrimental to obtaining HBsAg loss with PEG-IFN therapy in CHB patients.
Keywords: ACSL1; Chronic hepatitis B; HBsAg loss; Interferon-alfa; Liver steatosis; Triglyceride.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures






References
LinkOut - more resources
Full Text Sources
Miscellaneous
