

A Superior Squeeze: Superior Vena Cava Syndrome Secondary to Small Cell Lung Cancer
- PMID: 38975368
- PMCID: PMC11226217
- DOI: 10.7759/cureus.61717
A Superior Squeeze: Superior Vena Cava Syndrome Secondary to Small Cell Lung Cancer
Abstract
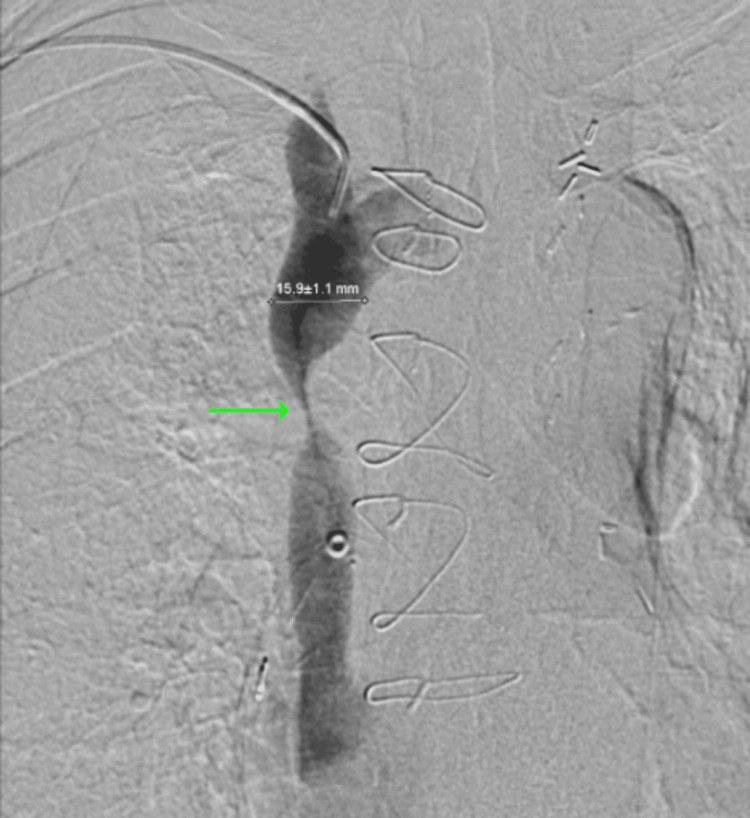
Superior vena cava (SVC) syndrome is an uncommon yet potentially fatal syndrome occurring after intrinsic or extrinsic compression to the SVC. While there are multiple emerging etiologies for this phenomenon, malignancy remains the most common. It is characterized by several symptoms including facial swelling, extremity swelling, shortness of breath, and headaches. We present the case of a 59-year-old female with a past medical history of cocaine abuse who was admitted for upper extremity swelling and facial edema. Imaging revealed a right suprahilar mass compressing a branch of the right pulmonary artery and SVC, in addition to bilateral segmental and subsegmental pulmonary emboli. She underwent an emergent biopsy and SVC stenting, with immunostaining revealing small cell lung cancer (SCLC). This case highlights a severe presentation of SVC syndrome caused by previously undetected SCLC.
Keywords: facial edema; interventional radiology stent placement; lung cancer; lung cancer surveillance; pulmonary embolism (pe); small-cell lung carcinoma; superior vena cava (svc) syndrome; tobacco adverse effects; venography; venoplasty.
Copyright © 2024, Reddy et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures








References
-
- Seligson M, Surowiec S. StatPearls. Treasure Island (FL): StatPearls Publishing; 2022. Superior vena cava syndrome. - PubMed
-
- Superior vena cava syndrome. Azizi AH, Shafi I, Shah N, Rosenfield K, Schainfeld R, Sista A, Bashir R. JACC Cardiovasc Interv. 2020;13:2896–2910. - PubMed
-
- Superior vena cava syndrome with malignant causes. Wilson LD, Detterbeck FC, Yahalom J. N Engl J Med. 2007;356:1862–1869. - PubMed
-
- The superior vena cava syndrome: clinical characteristics and evolving etiology. Rice TW, Rodriguez RM, Light RW. Medicine (Baltimore) 2006;85:37–42. - PubMed
-
- Superior vena cava syndrome from extensive lung cancer. Prasad R, Kemnic T. J Osteopath Med. 2021;121:329–330. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous