

Semaglutide vs Tirzepatide for Weight Loss in Adults With Overweight or Obesity
- PMID: 38976257
- PMCID: PMC11231910
- DOI: 10.1001/jamainternmed.2024.2525
Semaglutide vs Tirzepatide for Weight Loss in Adults With Overweight or Obesity
Abstract
Importance: Although tirzepatide and semaglutide were shown to reduce weight in randomized clinical trials, data from head-to-head comparisons in populations with overweight or obesity are not yet available.
Objective: To compare on-treatment weight loss and rates of gastrointestinal adverse events (AEs) among adults with overweight or obesity receiving tirzepatide or semaglutide labeled for type 2 diabetes (T2D) in a clinical setting.
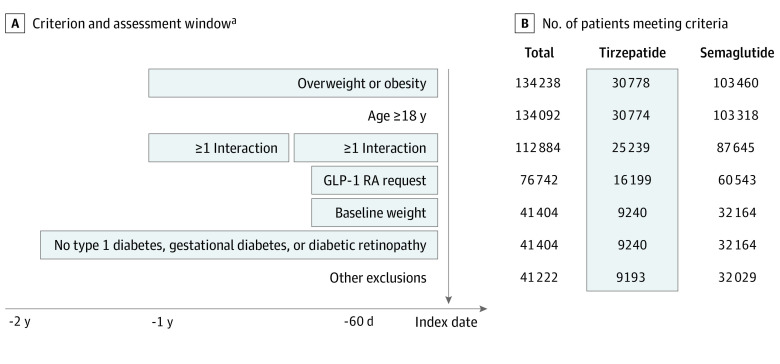
Design, setting, and participants: In this cohort study, adults with overweight or obesity receiving semaglutide or tirzepatide between May 2022 and September 2023 were identified using electronic health record (EHR) data linked to dispensing information from a collective of US health care systems. On-treatment weight outcomes through November 3, 2023, were assessed. Adults with overweight or obesity and regular care in the year before initiation, no prior glucagon-like peptide 1 receptor agonist receptor agonist use, a prescription within 60 days prior to initiation, and an available baseline weight were identified. The analysis was completed on April 3, 2024.
Exposures: Tirzepatide or semaglutide in formulations labeled for T2D, on or off label.
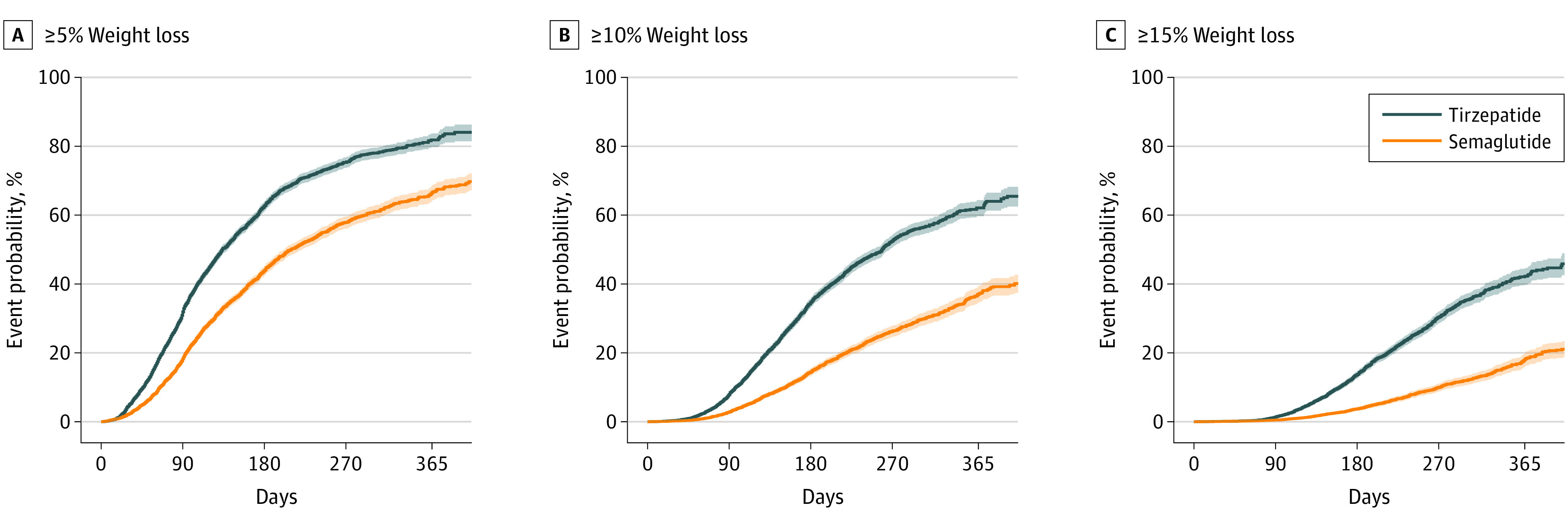
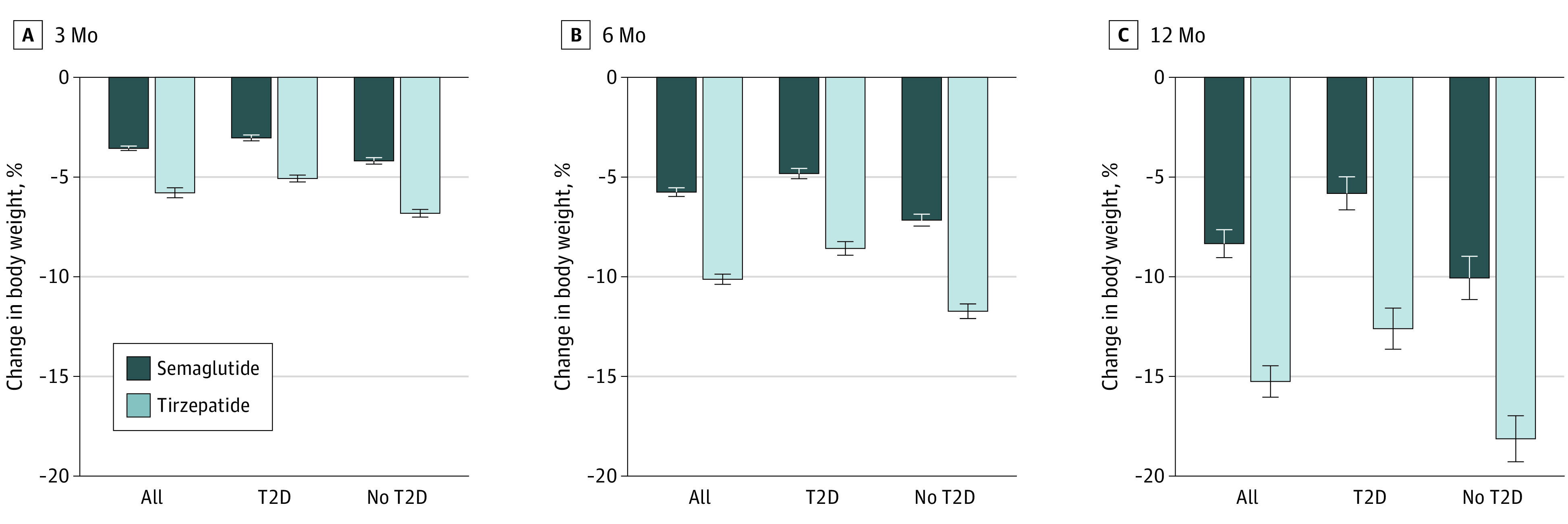
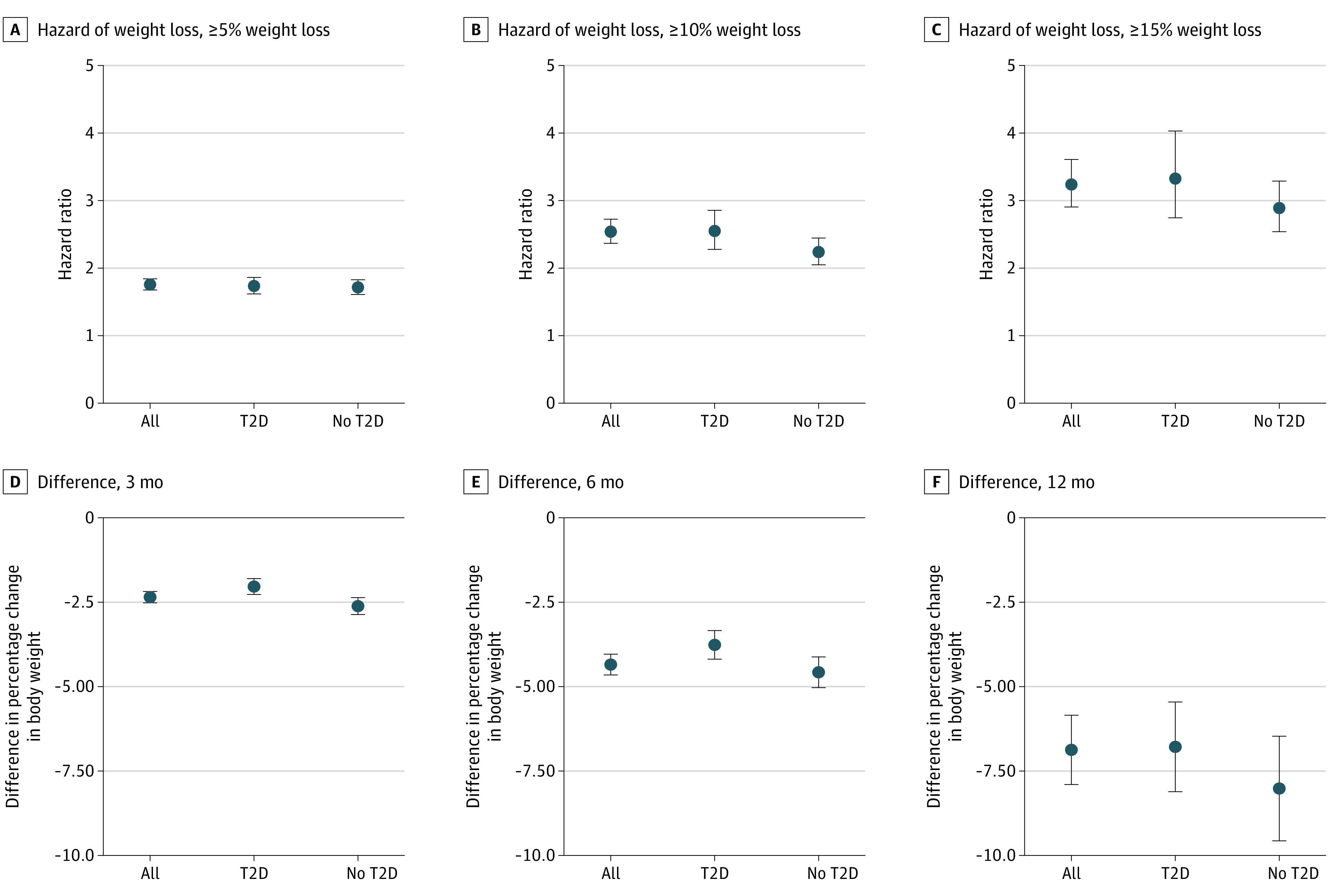
Main outcomes and measures: On-treatment weight change in a propensity score-matched population, assessed as hazard of achieving 5% or greater, 10% or greater, and 15% or greater weight loss, and percentage change in weight at 3, 6, and 12 months. Hazards of gastrointestinal AEs were compared.
Results: Among 41 222 adults meeting the study criteria (semaglutide, 32 029; tirzepatide, 9193), 18 386 remained after propensity score matching. The mean (SD) age was 52.0 (12.9) years, 12 970 were female (70.5%), 14 182 were white (77.1%), 2171 Black (11.8%), 354 Asian (1.9%), 1679 were of other or unknown race, and 9563 (52.0%) had T2D. The mean (SD) baseline weight was 110 (25.8) kg. Follow-up was ended by discontinuation for 5140 patients (55.9%) receiving tirzepatide and 4823 (52.5%) receiving semaglutide. Patients receiving tirzepatide were significantly more likely to achieve weight loss (≥5%; hazard ratio [HR], 1.76, 95% CI, 1.68, 1.84; ≥10%; HR, 2.54; 95% CI, 2.37, 2.73; and ≥15%; HR, 3.24; 95% CI, 2.91, 3.61). On-treatment changes in weight were larger for patients receiving tirzepatide at 3 months (difference, -2.4%; 95% CI -2.5% to -2.2%), 6 months (difference, -4.3%; 95% CI, -4.7% to -4.0%), and 12 months (difference, -6.9%; 95% CI, -7.9% to -5.8%). Rates of gastrointestinal AEs were similar between groups.
Conclusions and relevance: In this population of adults with overweight or obesity, use of tirzepatide was associated with significantly greater weight loss than semaglutide. Future study is needed to understand differences in other important outcomes.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
