

Comparative Effectiveness and Safety of Apixaban, Rivaroxaban, and Warfarin in Patients With Cirrhosis and Atrial Fibrillation : A Nationwide Cohort Study
- PMID: 38976880
- PMCID: PMC11671173
- DOI: 10.7326/M23-3067
Comparative Effectiveness and Safety of Apixaban, Rivaroxaban, and Warfarin in Patients With Cirrhosis and Atrial Fibrillation : A Nationwide Cohort Study
Abstract
Background: Apixaban, rivaroxaban, and warfarin have shown benefit for preventing major ischemic events, albeit with increased bleeding risk, among patients in the general population with atrial fibrillation (AF). However, data are scarce in patients with cirrhosis and AF.
Objective: To compare the effectiveness and safety of apixaban versus rivaroxaban and versus warfarin in patients with cirrhosis and AF.
Design: Population-based cohort study.
Setting: Two U.S. claims data sets (Medicare and Optum's de-identified Clinformatics Data Mart Database [2013 to 2022]).
Participants: 1:1 propensity score (PS)-matched patients with cirrhosis and nonvalvular AF initiating use of apixaban, rivaroxaban, or warfarin.
Measurements: Primary outcomes included ischemic stroke or systemic embolism and major hemorrhage (intracranial hemorrhage or major gastrointestinal bleeding). Database-specific and pooled PS-matched rate differences (RDs) per 1000 person-years (PY) and Cox proportional hazard ratios (HRs) with 95% CIs were estimated, controlling for 104 preexposure covariates.
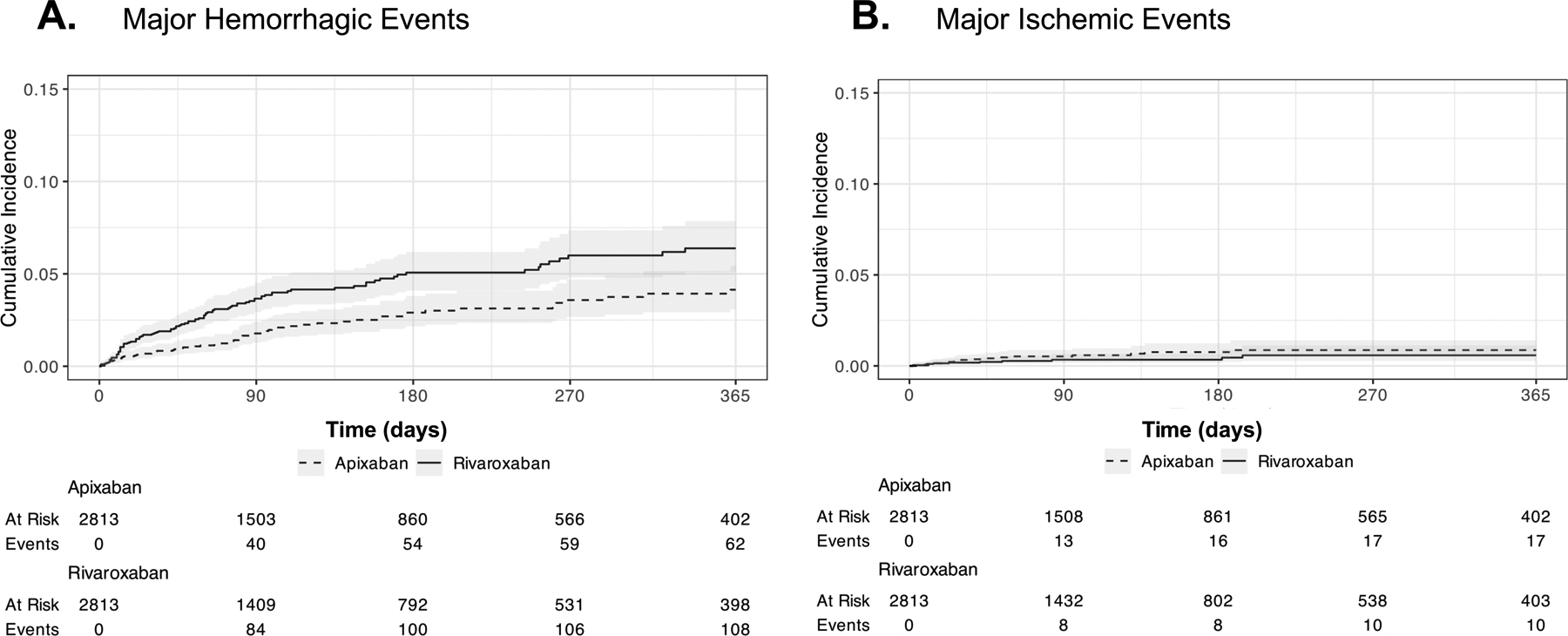
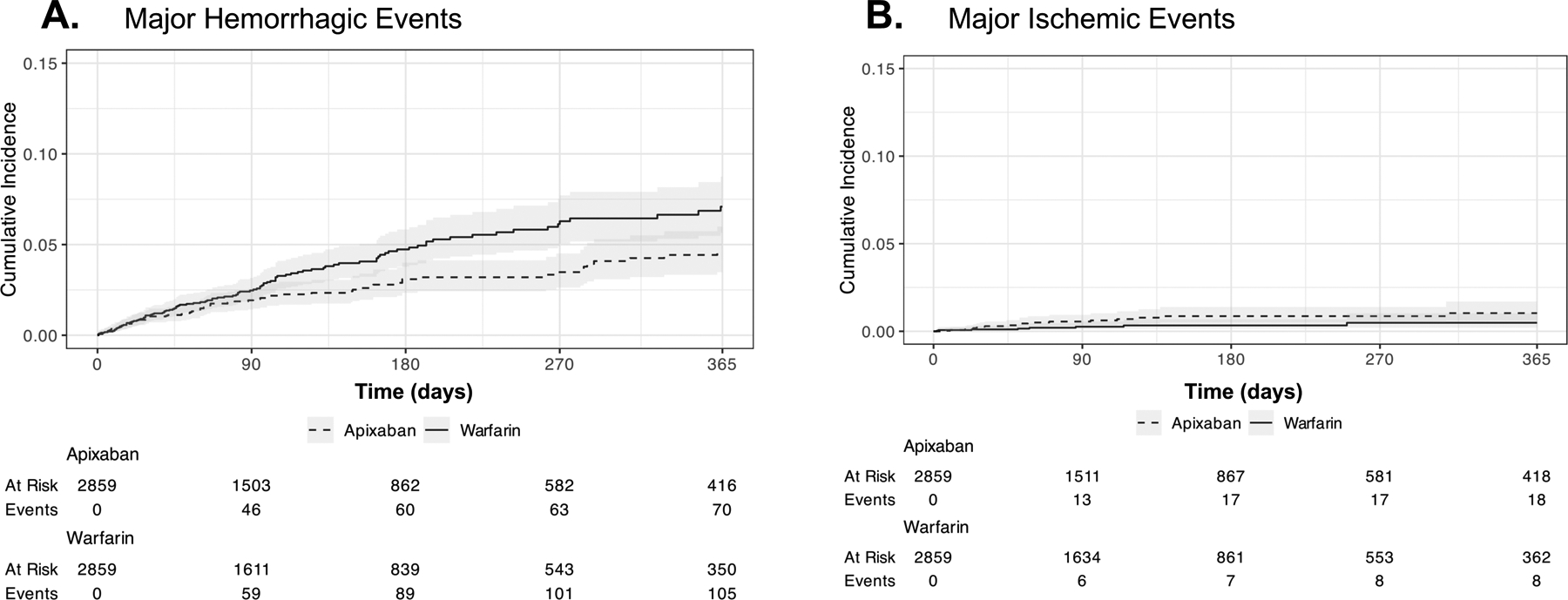
Results: Rivaroxaban initiators had significantly higher rates of major hemorrhagic events than apixaban initiators (RD, 33.1 per 1000 PY [95% CI, 12.9 to 53.2 per 1000 PY]; HR, 1.47 [CI, 1.11 to 1.94]) but no significant differences in rates of ischemic events or death. Consistently higher rates of major hemorrhage were found with rivaroxaban across subgroup and sensitivity analyses. Warfarin initiators also had significantly higher rates of major hemorrhage than apixaban initiators (RD, 26.1 per 1000 PY [CI, 6.8 to 45.3 per 1000 PY]; HR, 1.38 [CI, 1.03 to 1.84]), particularly hemorrhagic stroke (RD, 9.7 per 1000 PY [CI, 2.2 to 17.2 per 1000 PY]; HR, 2.85 [CI, 1.24 to 6.59]).
Limitation: Nonrandomized treatment selection.
Conclusion: Among patients with cirrhosis and nonvalvular AF, initiators of rivaroxaban versus apixaban had significantly higher rates of major hemorrhage and similar rates of ischemic events and death. Initiation of warfarin versus apixaban also contributed to significantly higher rates of major hemorrhagic events, including hemorrhagic stroke.
Primary funding source: National Institutes of Health.
Conflict of interest statement
Figures
Similar articles
-
Association of Rivaroxaban vs Apixaban With Major Ischemic or Hemorrhagic Events in Patients With Atrial Fibrillation.JAMA. 2021 Dec 21;326(23):2395-2404. doi: 10.1001/jama.2021.21222. JAMA. 2021. PMID: 34932078 Free PMC article.
-
Comparative Safety and Effectiveness of Warfarin or Rivaroxaban Versus Apixaban in Patients With Advanced CKD and Atrial Fibrillation: Nationwide US Cohort Study.Am J Kidney Dis. 2024 Mar;83(3):293-305.e1. doi: 10.1053/j.ajkd.2023.08.017. Epub 2023 Oct 13. Am J Kidney Dis. 2024. PMID: 37839687 Free PMC article.
-
Effectiveness and Safety in Patients with Non-Valvular Atrial Fibrillation Who Switched from Warfarin to Direct Oral Anticoagulants in Medicare Population.Adv Ther. 2025 Mar;42(3):1462-1483. doi: 10.1007/s12325-024-03099-y. Epub 2025 Jan 30. Adv Ther. 2025. PMID: 39883308 Free PMC article.
-
Direct comparative effectiveness and safety between non-vitamin K antagonist oral anticoagulants for stroke prevention in nonvalvular atrial fibrillation: a systematic review and meta-analysis of observational studies.Eur J Epidemiol. 2019 Feb;34(2):173-190. doi: 10.1007/s10654-018-0415-7. Epub 2018 Jun 8. Eur J Epidemiol. 2019. PMID: 29948370
-
An indirect comparison of dabigatran, rivaroxaban and apixaban for atrial fibrillation.Thromb Haemost. 2012 Sep;108(3):476-84. doi: 10.1160/TH12-02-0093. Epub 2012 Jun 28. Thromb Haemost. 2012. PMID: 22740145 Review.
Cited by
-
New pharmacological agents and novel cardiovascular pharmacotherapy strategies in 2024.Eur Heart J Cardiovasc Pharmacother. 2025 May 2;11(3):292-317. doi: 10.1093/ehjcvp/pvaf012. Eur Heart J Cardiovasc Pharmacother. 2025. PMID: 40058879 Free PMC article. Review.
-
Effectiveness and safety of direct oral anticoagulants versus vitamin K antagonists in atrial fibrillation patients with liver disease: a systematic review and meta-analysis.Front Pharmacol. 2025 Jul 14;16:1620394. doi: 10.3389/fphar.2025.1620394. eCollection 2025. Front Pharmacol. 2025. PMID: 40727096 Free PMC article.
-
Comparison of the Efficacy and Safety of Direct Oral Anticoagulants and Warfarin in Cirrhotic Patients: A Systematic Review and Meta-Analysis.Clin Appl Thromb Hemost. 2024 Jan-Dec;30:10760296241301402. doi: 10.1177/10760296241301402. Clin Appl Thromb Hemost. 2024. PMID: 39552309 Free PMC article.
-
Bleeding Complications Following Paracentesis in Patients Taking Apixaban.Cureus. 2025 Mar 9;17(3):e80299. doi: 10.7759/cureus.80299. eCollection 2025 Mar. Cureus. 2025. PMID: 40201875 Free PMC article.
References
-
- Asrani SK, Devarbhavi H, Eaton J, Kamath PS. Burden of liver diseases in the world. J Hepatol. 2019;70(1):151–71. - PubMed
-
- Chokesuwattanaskul R, Thongprayoon C, Bathini T, O’Corragain OA, Sharma K, Preechawat S, et al. Epidemiology of atrial fibrillation in patients with cirrhosis and clinical significance: a meta-analysis. Eur J Gastroenterol Hepatol. 2019;31(4):514–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous