

Empagliflozin rescues pro-arrhythmic and Ca2+ homeostatic effects of transverse aortic constriction in intact murine hearts
- PMID: 38977794
- PMCID: PMC11231339
- DOI: 10.1038/s41598-024-66098-7
Empagliflozin rescues pro-arrhythmic and Ca2+ homeostatic effects of transverse aortic constriction in intact murine hearts
Abstract
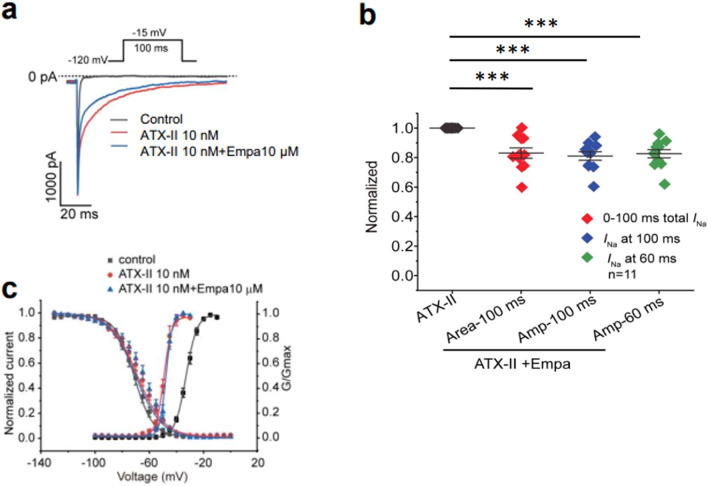
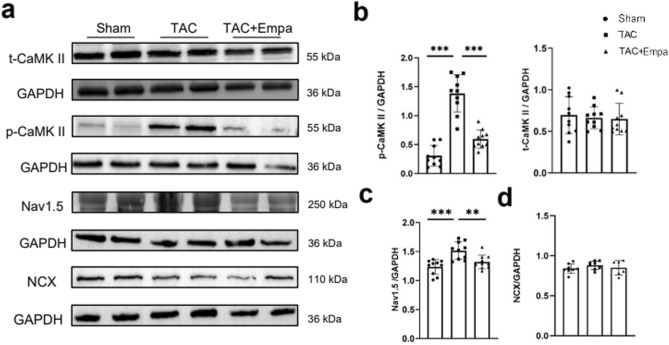
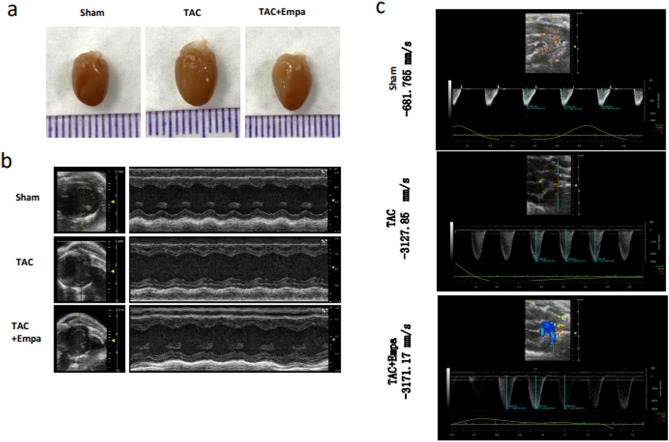
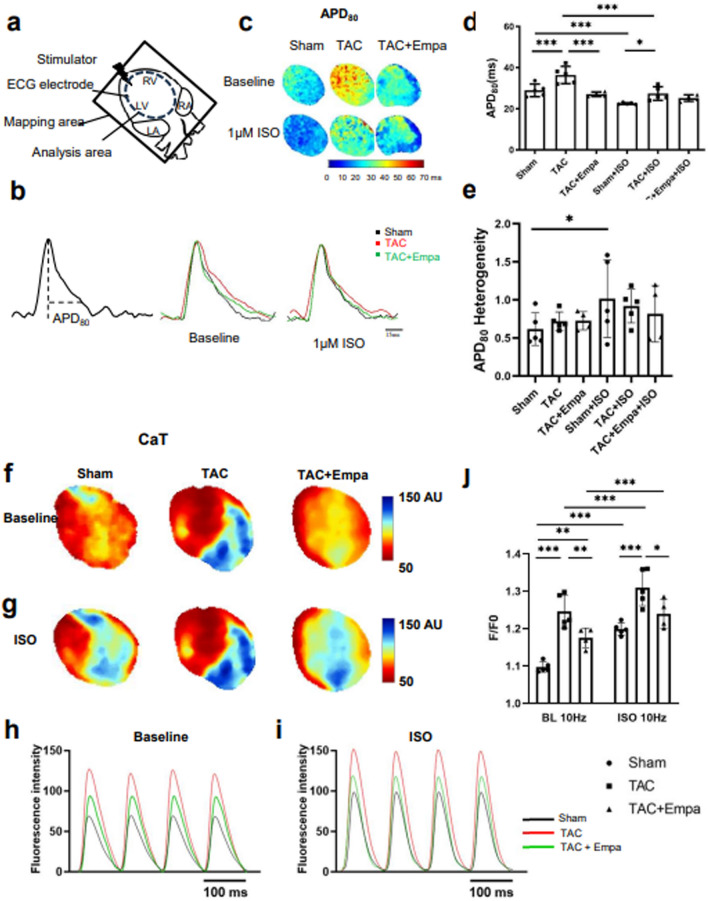
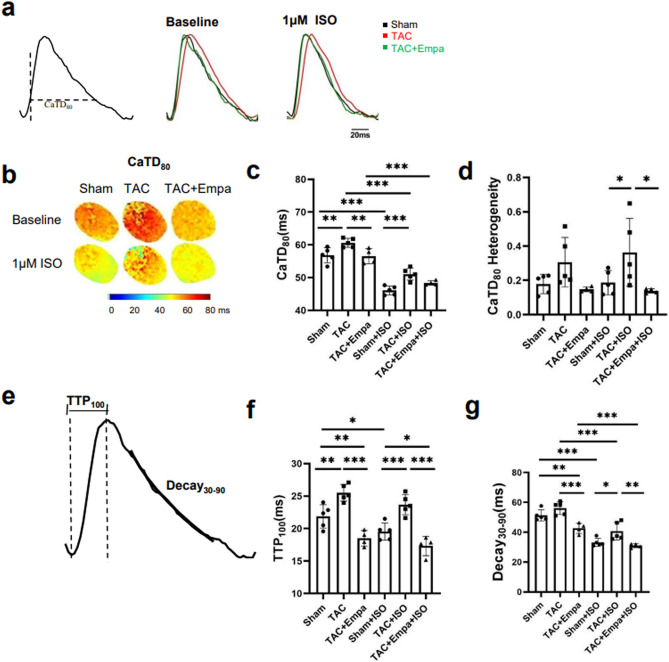
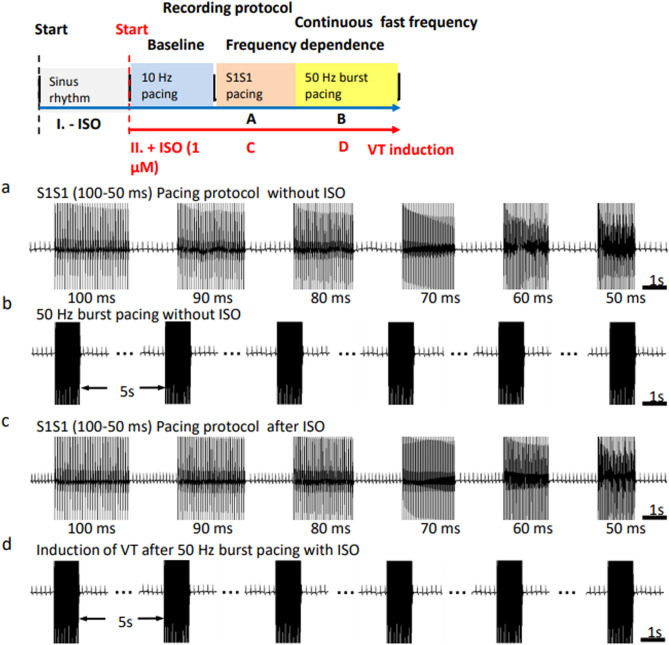
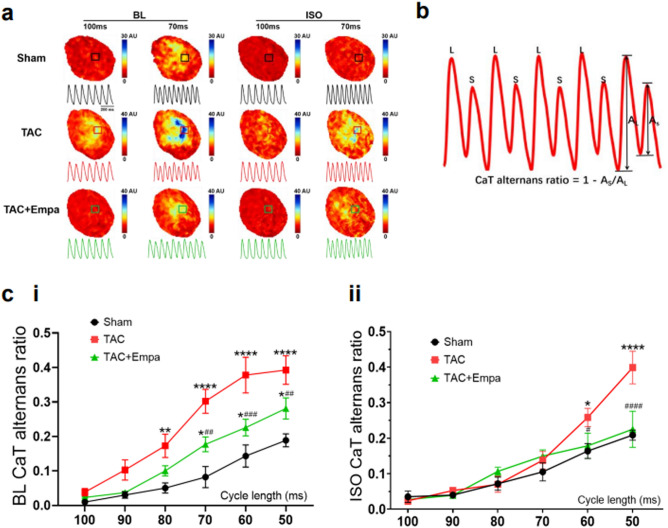
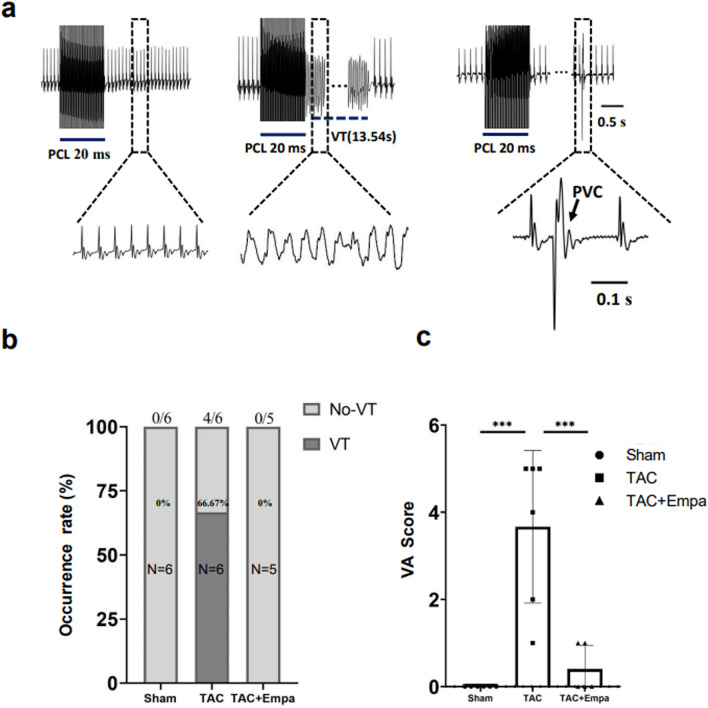
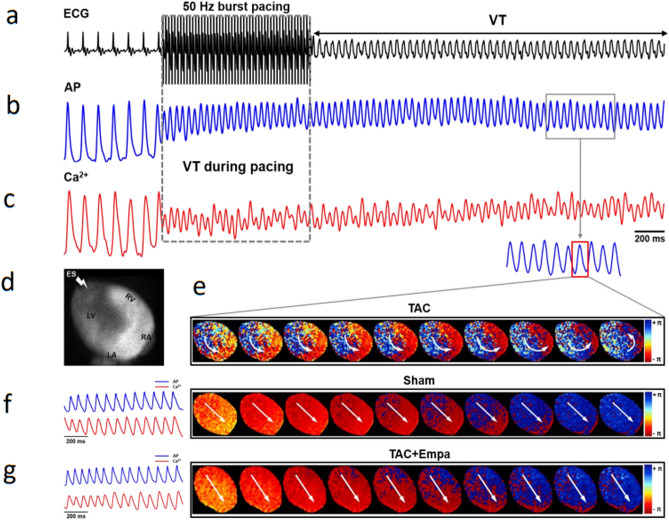
We explored physiological effects of the sodium-glucose co-transporter-2 inhibitor empagliflozin on intact experimentally hypertrophic murine hearts following transverse aortic constriction (TAC). Postoperative drug (2-6 weeks) challenge resulted in reduced late Na+ currents, and increased phosphorylated (p-)CaMK-II and Nav1.5 but not total (t)-CaMK-II, and Na+/Ca2+ exchanger expression, confirming previous cardiomyocyte-level reports. It rescued TAC-induced reductions in echocardiographic ejection fraction and fractional shortening, and diastolic anterior and posterior wall thickening. Dual voltage- and Ca2+-optical mapping of Langendorff-perfused hearts demonstrated that empagliflozin rescued TAC-induced increases in action potential durations at 80% recovery (APD80), Ca2+ transient peak signals and durations at 80% recovery (CaTD80), times to peak Ca2+ (TTP100) and Ca2+ decay constants (Decay30-90) during regular 10-Hz stimulation, and Ca2+ transient alternans with shortening cycle length. Isoproterenol shortened APD80 in sham-operated and TAC-only hearts, shortening CaTD80 and Decay30-90 but sparing TTP100 and Ca2+ transient alternans in all groups. All groups showed similar APD80, and TAC-only hearts showed greater CaTD80, heterogeneities following isoproterenol challenge. Empagliflozin abolished or reduced ventricular tachycardia and premature ventricular contractions and associated re-entrant conduction patterns, in isoproterenol-challenged TAC-operated hearts following successive burst pacing episodes. Empagliflozin thus rescues TAC-induced ventricular hypertrophy and systolic functional, Ca2+ homeostatic, and pro-arrhythmogenic changes in intact hearts.
Keywords: Action potential duration; Ca2+ homeostasis; Empagliflozin; Heart failure; Transverse aortic constriction (TAC); Ventricular arrhythmia.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
