

A multicenter study of asymmetric and symmetric dimethylarginine as predictors of mortality risk in hospitalized COVID-19 patients
- PMID: 38977837
- PMCID: PMC11231343
- DOI: 10.1038/s41598-024-66288-3
A multicenter study of asymmetric and symmetric dimethylarginine as predictors of mortality risk in hospitalized COVID-19 patients
Erratum in
-
Author Correction: A multicenter study of asymmetric and symmetric dimethylarginine as predictors of mortality risk in hospitalized COVID-19 patients.Sci Rep. 2025 Apr 29;15(1):15048. doi: 10.1038/s41598-025-99224-0. Sci Rep. 2025. PMID: 40301495 Free PMC article. No abstract available.
Abstract
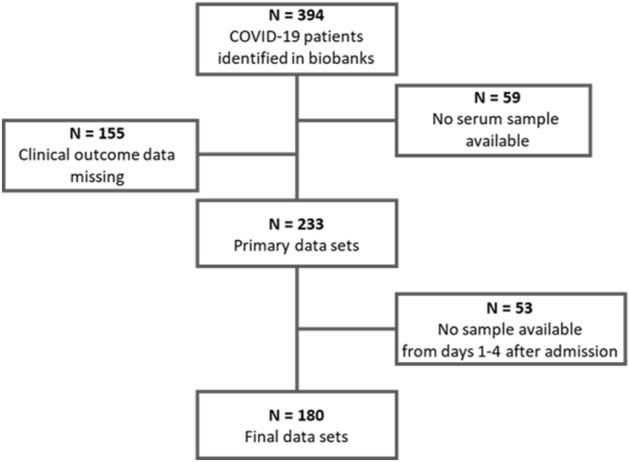
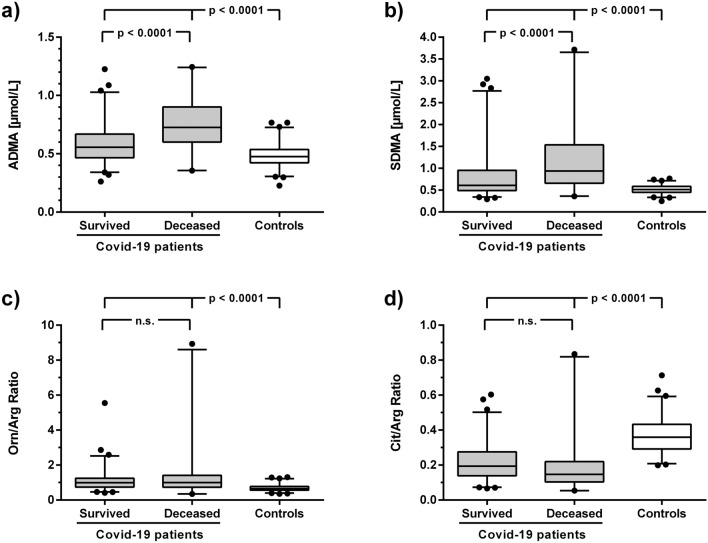
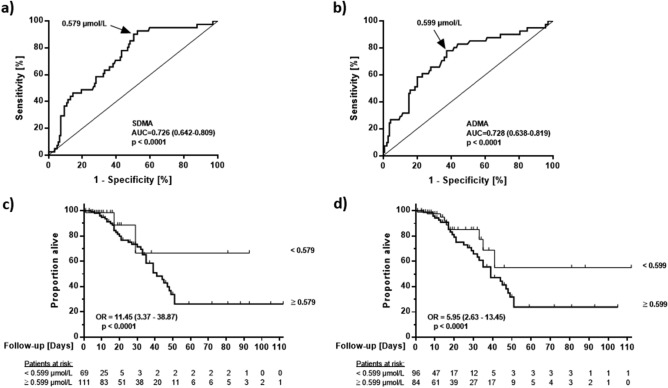
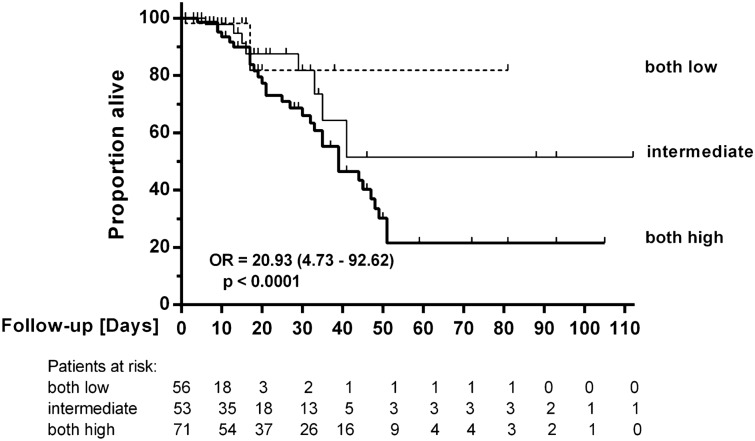
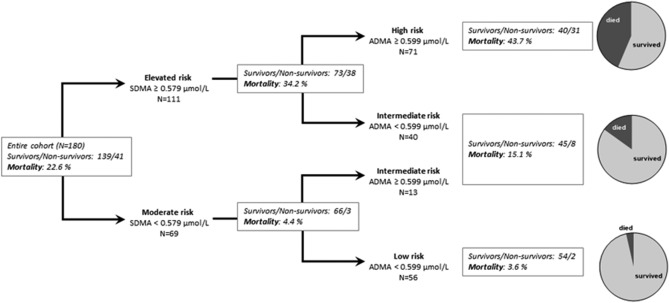
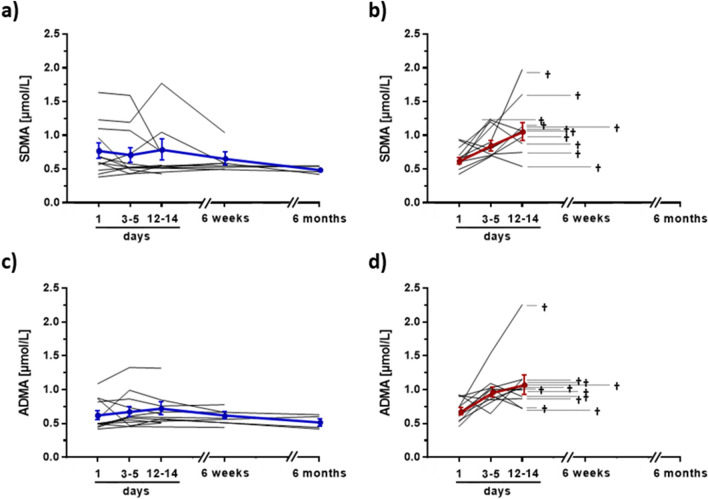
Mortality of patients hospitalized with COVID-19 has remained high during the consecutive SARS-CoV-2 pandemic waves. Early discrimination of patients at high mortality risk is crucial for optimal patient care. Symmetric (SDMA) and asymmetric dimethylarginine (ADMA) have been proposed as possible biomarkers to improve risk prediction of COVID-19 patients. We measured SDMA, ADMA, and other L-arginine-related metabolites in 180 patients admitted with COVID-19 in four German university hospitals as compared to 127 healthy controls. Patients were treated according to accepted clinical guidelines and followed-up until death or hospital discharge. Classical inflammatory markers (leukocytes, CRP, PCT), renal function (eGFR), and clinical scores (SOFA) were taken from hospital records. In a small subgroup of 23 COVID-19 patients, sequential blood samples were available and analyzed for biomarker trends over time until 14 days after admission. Patients had significantly elevated SDMA, ADMA, and L-ornithine and lower L-citrulline concentrations than controls. Within COVID-19 patients, SDMA and ADMA were significantly higher in non-survivors (n = 41, 22.8%) than in survivors. In ROC analysis, the optimal cut-off to discriminate non-survivors from survivors was 0.579 µmol/L for SDMA and 0.599 µmol/L for ADMA (both p < 0.001). High SDMA and ADMA were associated with odds ratios for death of 11.45 (3.37-38.87) and 5.95 (2.63-13.45), respectively. Analysis of SDMA and ADMA allowed discrimination of a high-risk (mortality, 43.7%), medium-risk (15.1%), and low-risk group (3.6%); risk prediction was significantly improved over classical laboratory markers. We conclude that analysis of ADMA and SDMA after hospital admission significantly improves risk prediction in COVID-19.
Keywords: Biomarker; Infectious diseases; Intensive care; Nitric oxide.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Gray, W. K., Navaratnam, A. V., Day, J., Wendon, J. & Briggs, T. W. R. COVID-19 hospital activity and in-hospital mortality during the first and second waves of the pandemic in England: An observational study. Thorax77(11), 1113–1120 (2022). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
