

Value-based preoperative assessment in a large academic hospital
- PMID: 38978057
- PMCID: PMC11232329
- DOI: 10.1186/s44158-024-00161-7
Value-based preoperative assessment in a large academic hospital
Erratum in
-
Correction: Value-based preoperative assessment in a large academic hospital.J Anesth Analg Crit Care. 2024 Jul 30;4(1):49. doi: 10.1186/s44158-024-00184-0. J Anesth Analg Crit Care. 2024. PMID: 39080723 Free PMC article. No abstract available.
Abstract
Background: Value-based healthcare (VBHC) is an approach that focuses on delivering the highest possible value for patients while driving cost efficiency in health services. It emphasizes improving patient outcomes and experiences while optimizing the use of resources, shifting the healthcare system's focus from the volume of services to the value delivered. Our study assessed the effectiveness of implementing a VBHC-principled, tailored preoperative evaluation in enhancing patient care and outcomes, as well as reducing healthcare costs.
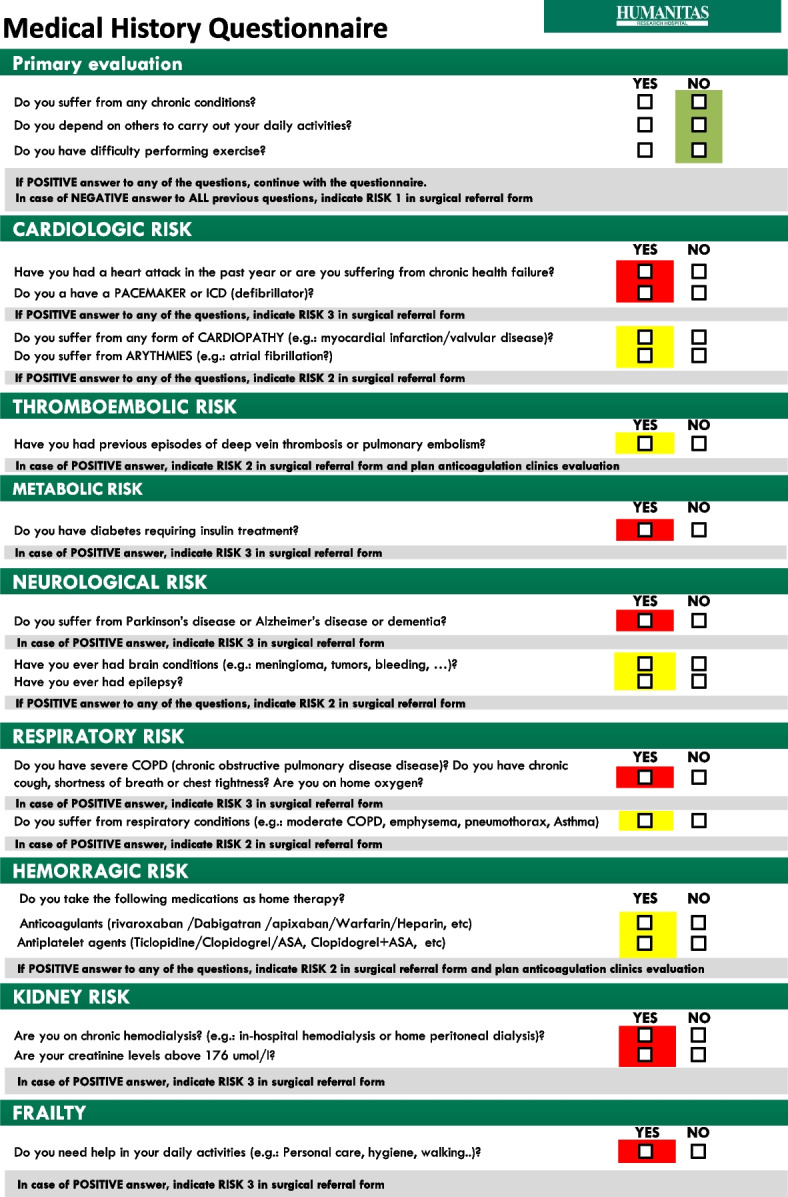
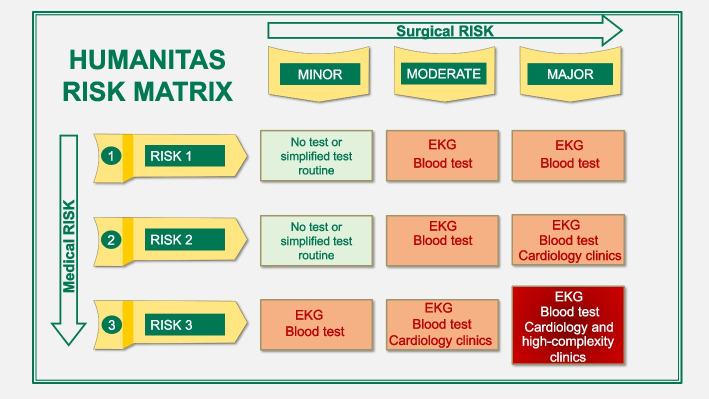
Methods: We employed a quality improvement, before-and-after approach to assessing the effects of implementing VBHC strategies on the restructuring of the preoperative evaluation clinics at Humanitas Research Hospital. The intervention introduced a VBHC-tailored risk matrix during the postintervention phase (year 2021), and the results were compared with those of the preintervention phase (2019). The primary study outcome was the difference in the number of preoperative tests and visits at baseline and after the VBHC approach. Secondary outcomes were patient outcomes and costs.
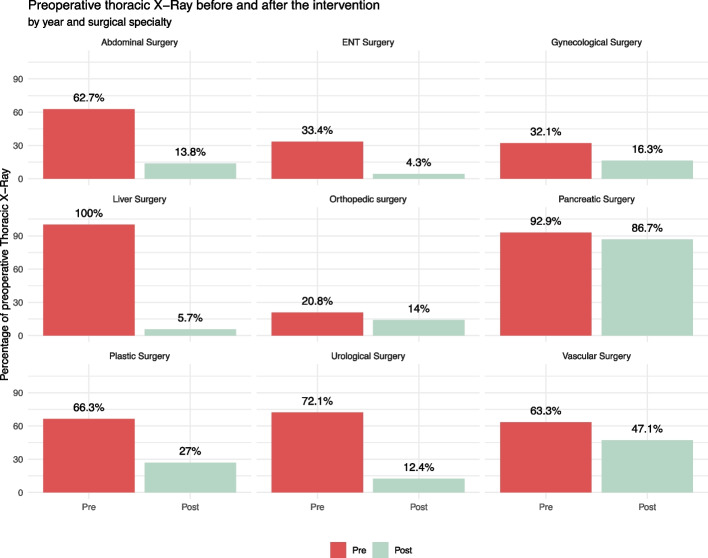
Results: A total of 9722 patients were included: 5242 during 2019 (baseline) and 4,480 during 2021 (VBHC approach). The median age of the population was 63 (IQR 51-72), 23% of patients were classified as ASA 3 and 4, and 26.8% (2,955 cases) were day surgery cases. We found a considerable decrease in the number of preoperative tests ordered for each patient [6.2 (2.5) vs 5.3 (2.6) tests, p < 0.001]. The number of preoperative chest X-ray, electrocardiogram, and cardiac exams decreased significantly with VBHC. The length of the preoperative evaluation was significantly shorter with VBHC [373 (136) vs 290 (157) min, p < 0.001]. Cost analysis demonstrated a significant reduction in costs, while there was no difference in clinical outcomes.
Conclusions: We demonstrated the feasibility, safety, and cost-effectiveness of a tailored approach for preoperative evaluation. The implementation of VBHC enhanced value, as evidenced by decreased patient time in preoperative evaluation and by a reduction in unnecessary preoperative tests.
Keywords: Outcomes; Patient empowerment; Patient-centred care; Preoperative assessment; Preoperative evaluation; Quality; Risk; Surgery; Value-based healthcare.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Hillary W, Justin G, Bharat M, Jitendra M (2016) Value based Healthcare. Advances In Management. p 9