

This is a preprint.
Multi-omic analysis of SDHB-deficient pheochromocytomas and paragangliomas identifies metastasis and treatment-related molecular profiles
- PMID: 38978571
- PMCID: PMC11230496
- DOI: 10.21203/rs.3.rs-4410500/v1
Multi-omic analysis of SDHB-deficient pheochromocytomas and paragangliomas identifies metastasis and treatment-related molecular profiles
Update in
-
Multi-omic analysis of SDHB-deficient pheochromocytomas and paragangliomas identifies metastasis and treatment-related molecular profiles.Nat Commun. 2025 Mar 17;16(1):2632. doi: 10.1038/s41467-025-57595-y. Nat Commun. 2025. PMID: 40097403 Free PMC article.
Abstract
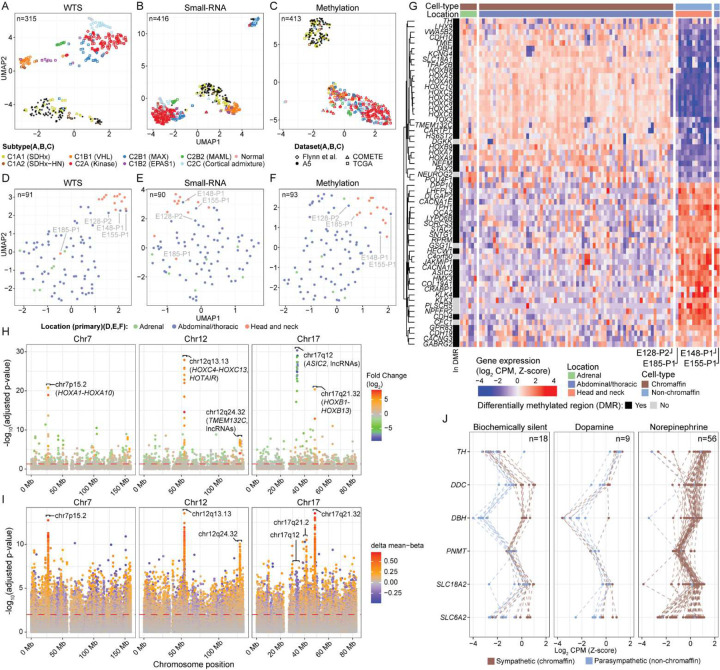
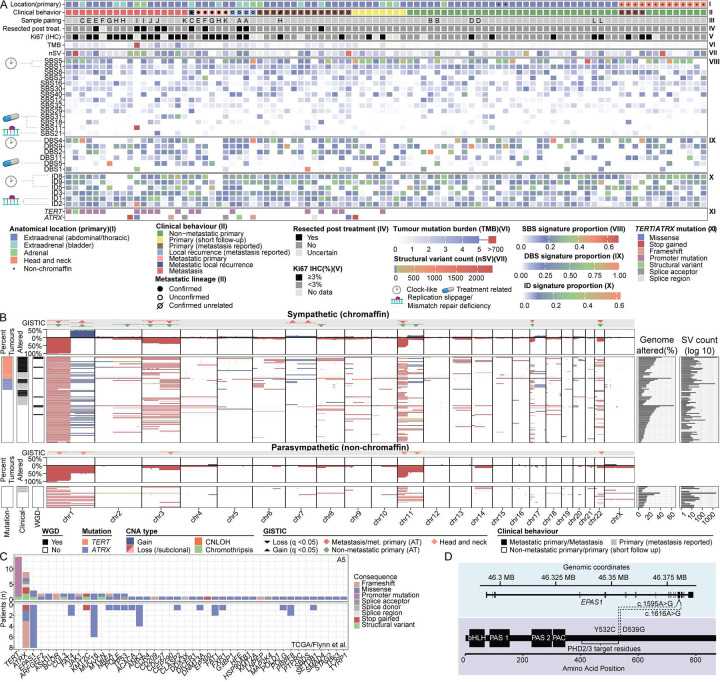
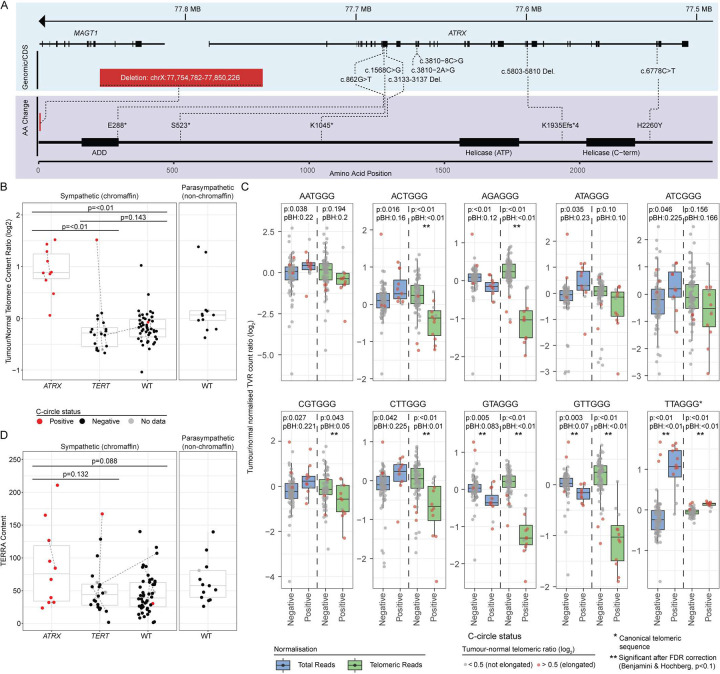
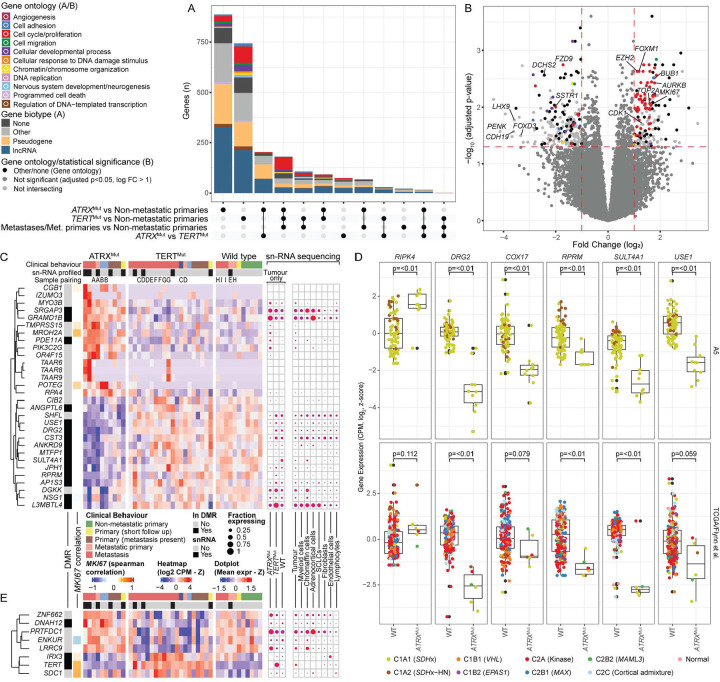
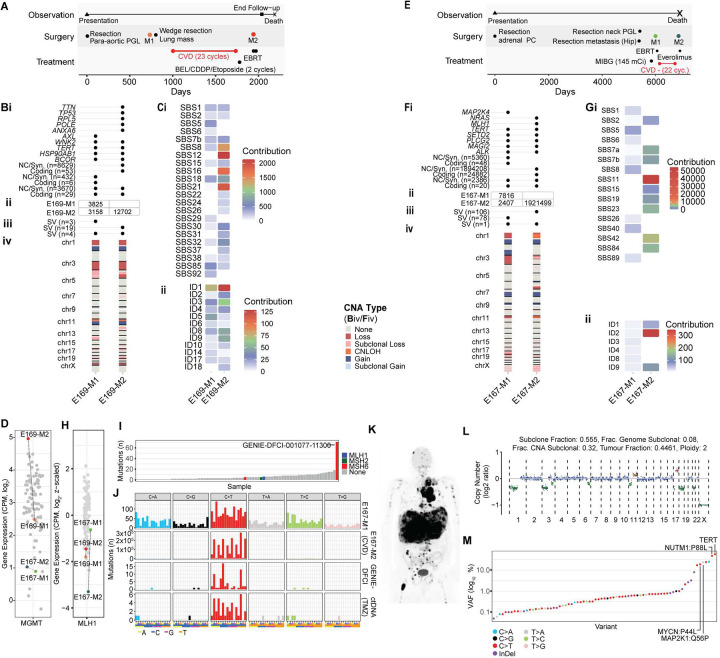
Hereditary SDHB-mutant pheochromocytomas (PC) and paragangliomas (PG) are rare tumours with a high propensity to metastasize although their clinical behaviour is unpredictable. To characterize the genomic landscape of these tumours and identify metastasis biomarkers, we performed multi-omic analysis on 94 tumours from 79 patients using seven molecular methods. Sympathetic (chromaffin cell) and parasympathetic (non-chromaffin cell) PCPG had distinct molecular profiles reflecting their cell-of-origin and biochemical profile. TERT and ATRX-alterations were associated with metastatic PCPG and these tumours had an increased mutation load, and distinct transcriptional and telomeric features. Most PCPG had quiet genomes with some rare co-operative driver events observed, including EPAS1/HIF-2α mutations. Two mechanisms of acquired resistance to DNA alkylating chemotherapies were also detected - MGMT overexpression and mismatch repair-deficiency causing hypermutation. Our comprehensive multi-omic analysis of SDHB-mutant PCPG therefore identified features of metastatic disease and treatment response, expanding our understanding of these rare neuroendocrine tumours.
Conflict of interest statement
Competing interests The authors declare no competing interests.
Figures



References
-
- Nazari M.A., et al. Catecholamine-induced hypertensive crises: current insights and management. Lancet Diabetes Endocrinol 11, 942–954 (2023). - PubMed
-
- Lenders J.W., Eisenhofer G., Mannelli M. & Pacak K. Phaeochromocytoma. Lancet 366, 665–675 (2005). - PubMed
-
- Ayala-Ramirez M., et al. Clinical risk factors for malignancy and overall survival in patients with pheochromocytomas and sympathetic paragangliomas: primary tumor size and primary tumor location as prognostic indicators. J Clin Endocrinol Metab 96, 717–725 (2011). - PubMed
-
- Lenders J.W.M., et al. Genetics, diagnosis, management and future directions of research of phaeochromocytoma and paraganglioma: a position statement and consensus of the Working Group on Endocrine Hypertension of the European Society of Hypertension. Journal of hypertension 38, 1443–1456 (2020). - PMC - PubMed
Publication types
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
