

Time from injury to acute surgery for patients with traumatic cervical spinal cord injury in South-East Norway
- PMID: 38978812
- PMCID: PMC11228170
- DOI: 10.3389/fneur.2024.1420530
Time from injury to acute surgery for patients with traumatic cervical spinal cord injury in South-East Norway
Abstract
Background: The recommended treatment for cervical spinal cord injury (cSCI) is surgical decompression and stabilization within 24 h after injury. The aims of the study were to estimate our institutional compliance with this recommendation and identify potential factors associated with surgical delay.
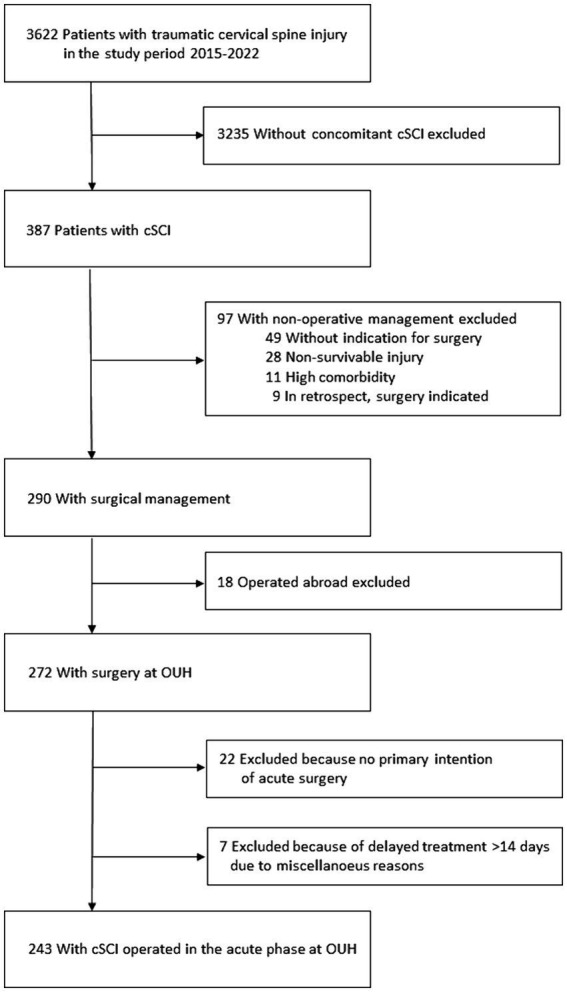
Methods: Population-based retrospective database study of patients operated for cSCI in 2015-2022 within the South-East Norway Health Region (3.1 million inhabitants). Data extracted were demographics, injury description, management timeline, place of primary triage [local hospital (LH) or neurotrauma center (NTC)]. Main outcome variables were: (1) time from injury to surgery at NTC, (2) time from injury to admission NTC, and (3) time from admission NTC to surgery.
Results: We found 243 cSCI patients having acute neck surgery. Their median age was 63 years (IQR 47-74 years), 77% were male, 48% were ≥65 years old. Primary triage at an LH occurred in 150/243 (62%). The median time from injury to acute surgery was 27.8 h (IQR 15.4-61.9 h), and 47% had surgery within 24 h. The median time from injury to NTC admission was 5.6 h (IQR 1.9-19.4 h), and 67% of the patients were admitted to the NTC within 12 h. Significant factors associated with increased time from injury to NTC admission were transfer via LH, severe preinjury comorbidities, less severe cSCI, time of injury other than night, absence of multiple injuries. The median time from NTC admission to surgery was 16.7 h (IQR 9.5-31.0 h), and 70% had surgery within 24 h. Significant factors associated with increased time from NTC admission to surgery were increasing age and non-translational injury morphology.
Conclusion: Less than half of the patients with cSCI were operated on within the recommended 24 h time frame after injury. To increase the fraction of early surgery, we suggest the following: (1) patients with clinical suspicion of cSCI should be transported directly to the NTC from the scene of the accident, (2) MRI should be performed only at the NTC, (3) at the NTC, surgery should commence on the same calendar day as arrival or as the first operation the following day.
Keywords: cervical spinal cord injury; improvement of care; neurotrauma; patient transfer; timing of surgery.
Copyright © 2024 Aarhus, Mirzamohammadi, Rønning, Strøm, Glott, Rizvi, Biernat, Ølstørn, Rydning, Stenset, Næss, Gaarder, Brommeland, Linnerud and Helseth.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Traumatic cervical spinal cord injury in southeastern Norway: acute treatment, specialized rehabilitation referral and mortality.Front Neurol. 2024 Dec 16;15:1452194. doi: 10.3389/fneur.2024.1452194. eCollection 2024. Front Neurol. 2024. PMID: 39737422 Free PMC article.
-
Admission ASIA motor score predicting the need for tracheostomy after cervical spinal cord injury.J Trauma Acute Care Surg. 2013 Oct;75(4):629-34. doi: 10.1097/TA.0b013e3182a12b86. J Trauma Acute Care Surg. 2013. PMID: 24064876
-
Can the acute magnetic resonance imaging features reflect neurologic prognosis in patients with cervical spinal cord injury?Spine J. 2017 Sep;17(9):1319-1324. doi: 10.1016/j.spinee.2017.05.009. Epub 2017 May 10. Spine J. 2017. PMID: 28501580
-
Influence of the timing of surgery for cervical spinal cord injury without bone injury in the elderly: A retrospective multicenter study.J Orthop Sci. 2024 Mar;29(2):480-485. doi: 10.1016/j.jos.2023.01.004. Epub 2023 Jan 29. J Orthop Sci. 2024. PMID: 36720671 Review.
-
Management of Cervical Spinal Cord Injury without Major Bone Injury in Adults.J Clin Med. 2023 Oct 27;12(21):6795. doi: 10.3390/jcm12216795. J Clin Med. 2023. PMID: 37959260 Free PMC article. Review.
Cited by
-
Traumatic cervical spinal cord injury in southeastern Norway: acute treatment, specialized rehabilitation referral and mortality.Front Neurol. 2024 Dec 16;15:1452194. doi: 10.3389/fneur.2024.1452194. eCollection 2024. Front Neurol. 2024. PMID: 39737422 Free PMC article.
-
Predictors of Early Mortality After Traumatic Spinal Cord Injury in South Africa.Global Spine J. 2025 May;15(4):2359-2366. doi: 10.1177/21925682241300269. Epub 2024 Nov 10. Global Spine J. 2025. PMID: 39523107 Free PMC article.
-
Epidemiology of Traumatic Cervical Spinal Cord Injury in Southeast Norway.Neurotrauma Rep. 2025 Jun 16;6(1):539-550. doi: 10.1089/neur.2025.0013. eCollection 2025. Neurotrauma Rep. 2025. PMID: 40630650 Free PMC article.
-
Management of traumatic spinal cord injury in the Nordic countries: a multidisciplinary survey.Scand J Trauma Resusc Emerg Med. 2025 Mar 24;33(1):51. doi: 10.1186/s13049-025-01349-8. Scand J Trauma Resusc Emerg Med. 2025. PMID: 40128803 Free PMC article.
References
-
- Fehlings MG, Vaccaro A, Wilson JR, Singh A, Cadotte D, Harrop JS, et al. . Early versus delayed decompression for traumatic cervical spinal cord injury: results of the surgical timing in acute spinal cord injury study (STASCIS). PLoS One. (2012) 7:e32037. doi: 10.1371/journal.pone.0032037, PMID: - DOI - PMC - PubMed
-
- Grassner L, Wutte C, Klein B, Mach O, Riesner S, Panzer S, et al. . Early decompression (< 8 h) after traumatic cervical spinal cord injury improves functional outcome as assessed by spinal cord independence measure after one year. J Neurotrauma. (2016) 33:1658–66. doi: 10.1089/neu.2015.4325, PMID: - DOI - PubMed
-
- Aarabi B, Akhtar-Danesh N, Simard JM, Chryssikos T, Shanmuganathan K, Olexa J, et al. . Efficacy of early (≤ 24 hours), late (25–72 hours), and delayed (>72 hours) surgery with magnetic resonance imaging-confirmed decompression in American spinal injury association impairment scale grades C and D acute traumatic central cord syndrome caused by spinal stenosis. J Neurotrauma. (2021) 38:2073–83. doi: 10.1089/neu.2021.0040, PMID: - DOI - PMC - PubMed
-
- Aarabi B, Akhtar-Danesh N, Chryssikos T, Shanmuganathan K, Schwartzbauer GT, Simard JM, et al. . Efficacy of ultra-early (< 12 h), early (12-24 h), and late (>24-138.5 h) surgery with magnetic resonance imaging-confirmed decompression in American spinal injury association impairment scale grades a, B, and C cervical spinal cord injury. J Neurotrauma. (2020) 37:448–57. doi: 10.1089/neu.2019.6606, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources