

Benefits of upgrading right ventricular to biventricular pacing in heart failure patients with atrial fibrillation
- PMID: 38979560
- PMCID: PMC11264293
- DOI: 10.1093/europace/euae179
Benefits of upgrading right ventricular to biventricular pacing in heart failure patients with atrial fibrillation
Abstract
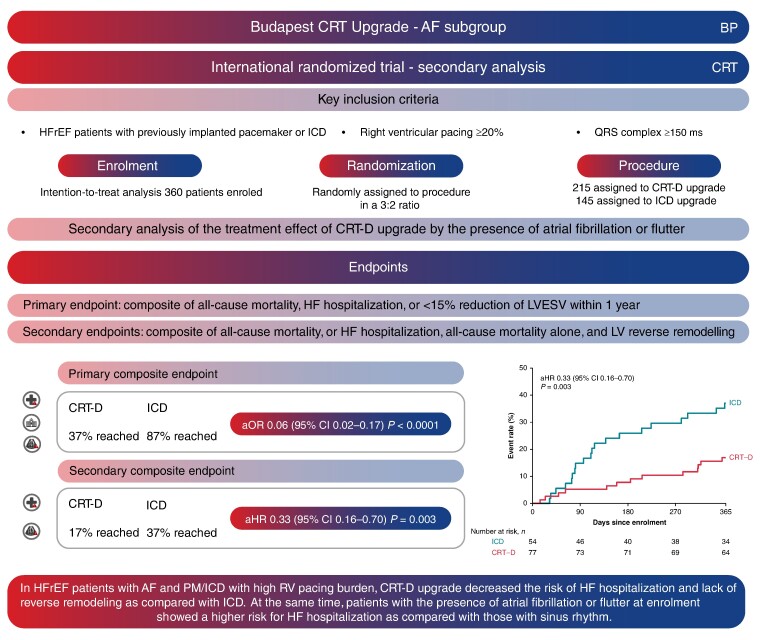
Aims: Recommendations on cardiac resynchronization therapy (CRT) in patients with atrial fibrillation or flutter (AF) are based on less robust evidence than those in sinus rhythm (SR). We aimed to assess the efficacy of CRT upgrade in the BUDAPEST-CRT Upgrade trial population by their baseline rhythm.
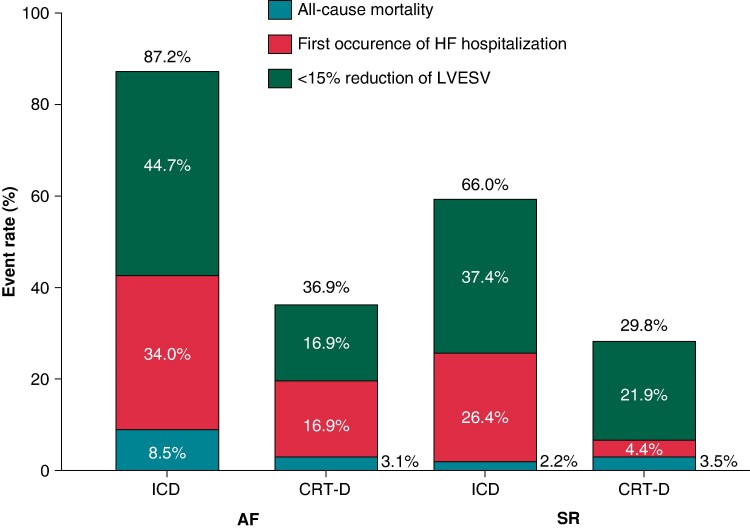
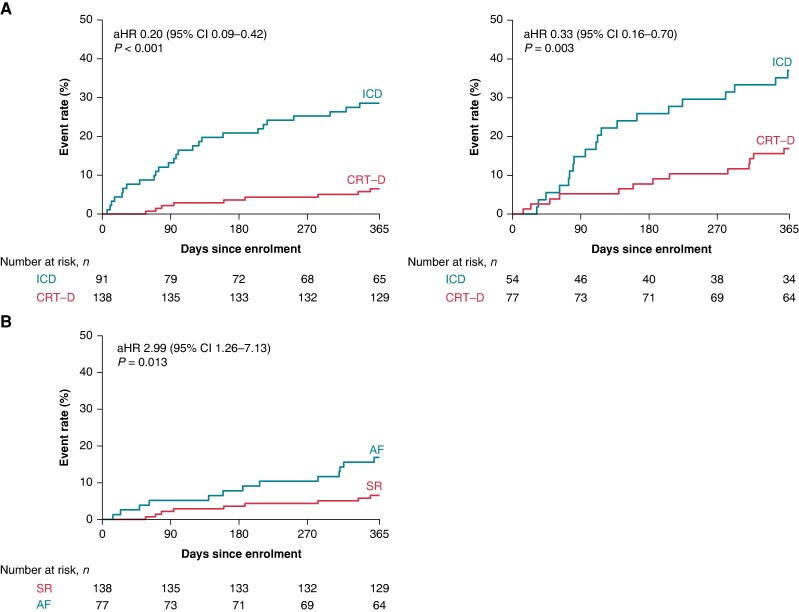
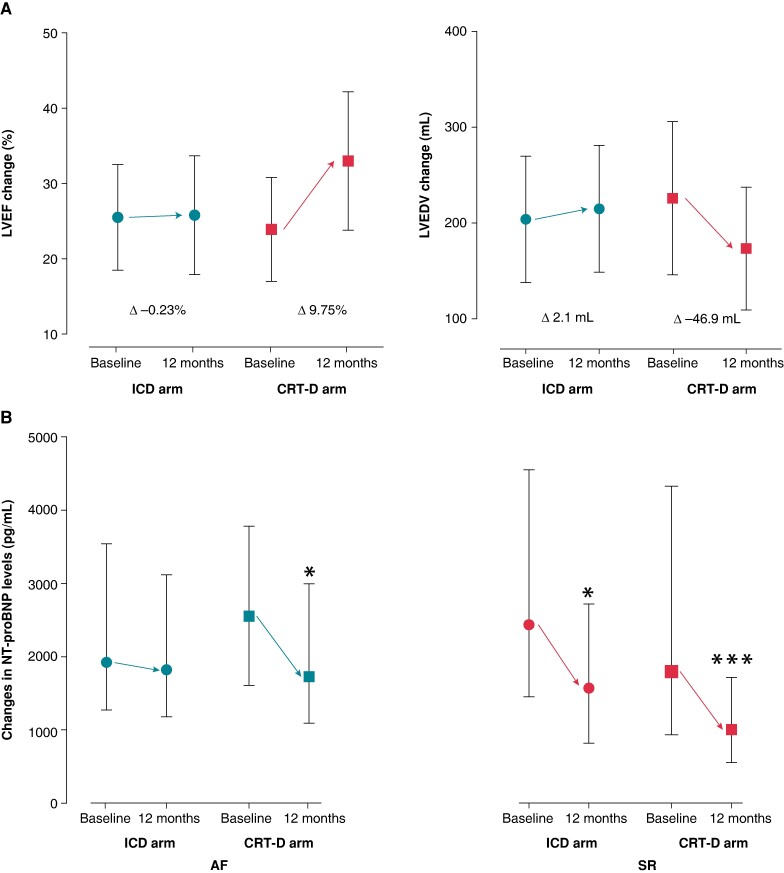
Methods and results: Heart failure patients with reduced ejection fraction (HFrEF) and previously implanted pacemaker (PM) or implantable cardioverter defibrillator (ICD) and ≥20% right ventricular (RV) pacing burden were randomized to CRT with defibrillator (CRT-D) upgrade (n = 215) or ICD (n = 145). Primary [HF hospitalization (HFH), all-cause mortality, or <15% reduction of left ventricular end-systolic volume] and secondary outcomes were investigated. At enrolment, 131 (36%) patients had AF, who had an increased risk for HFH as compared with those with SR [adjusted hazard ratio (aHR) 2.99; 95% confidence interval (CI) 1.26-7.13; P = 0.013]. The effect of CRT-D upgrade was similar in patients with AF as in those with SR [AF adjusted odds ratio (aOR) 0.06; 95% CI 0.02-0.17; P < 0.001; SR aOR 0.13; 95% CI 0.07-0.27; P < 0.001; interaction P = 0.29] during the mean follow-up time of 12.4 months. Also, it decreased the risk of HFH or all-cause mortality (aHR 0.33; 95% CI 0.16-0.70; P = 0.003; interaction P = 0.17) and improved the echocardiographic response (left ventricular end-diastolic volume difference -49.21 mL; 95% CI -69.10 to -29.32; P < 0.001; interaction P = 0.21).
Conclusion: In HFrEF patients with AF and PM/ICD with high RV pacing burden, CRT-D upgrade decreased the risk of HFH and improved reverse remodelling when compared with ICD, similar to that seen in patients in SR.
Keywords: Atrial fibrillation; Cardiac resynchronization therapy; Heart failure; Pacing-induced cardiomyopathy; Right ventricular pacing; Upgrade.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: B.M. reports grants from Boston Scientific, NRDIF Hungary, and National Heart Program during the conduct of the study; personal fees from Biotronik, Abbott, AstraZeneca, Novartis, and Boehringer Ingelheim; and grants from Medtronic outside the submitted work. I.O. reports lecture and advisory fees from Abbott, Biotronik, Boston Scientific, Medtronic, and Vitatron and travel grants from Abbott, Biotronik, Boston Scientific, and Medtronic. Attila K. reports grants from Bolyai Research Scholarship and FK ‘OTKA’ Research Grant from NKFIH outside the submitted work, stock from CardioSight, Inc. and stock option from Argus Cognitive, Inc. outside the submitted work, and personal fees from Argus Cognitive, Inc. and CardioSight Hungary LLC outside the submitted work. G.D. reports research grants to institution from Medtronic and Biotronik and lecture and advisory fees from Medtronic, Biotronik, and Abbott. C.F. reports support from the Semmelweis University, grants from Medtronic, consulting fees from Medtronic and Biotronik Hungary, and payment or honoraria for lectureures from Johnson and Johnson Co., Abbott Laboratories and Boehringer Ingelheim RCV GmbH and Co. L.G. reports support for the present manuscript from Vitatron Medical, Boston Scientific, Abbott Laboratories, Medtronic Hungary, and Biotronik Hungary; consulting fees from Medtronic Hungary and Abbott Hungary; honoraria; travel grants; participation on a data safety monitoring board or advisory board; and role in other board and committee (FESC, FEHRA, President of the Scientific Committee of the Hungarian Society of Cardiology, Past President of the Working Group on Cardiac Arrhythmias and Pacing, and EHRA Scientific Programme Board). Annamária K. reports grants from Bolyai Research Scholarship outside the submitted work; consulting fees from Medtronic; honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, Biotronik, and Novartis; payment for expert testimony from Boehringer Ingelheim and Boston Scientific; travel grants from AstraZeneca and Novartis; participation on a data safety monitoring board or advisory board for Boehringer Ingelheim and Boston Scientific; and role in other board and committee (committee member of Hungarian Society of Cardiology and secretary of the Working Group on Cardiac Arrhythmias and Pacing, Hungarian Society of Cardiology). S.D.S. reports grants to institution from Actelion, Alnylam, Amgen, AstraZeneca, Bellerophon, Bayer, BMS, Celladon, Cytokinetics, Eidos, Gilead, GSK, Ionis, Lilly, Mesoblast, MyoKardia, NIH/NHLBI, NeuroTronik, Novartis, Novo Nordisk, Respicardia, Sanofi Pasteur, Theracos, and US2.AI and consulting fees outside the scope of the current work from Abbott, Action, Akros, Alnylam, Amgen, Arena, AstraZeneca, Bayer, Boehringer Ingelheim, BMS, Cardior, Cardurion, Corvia, Cytokinetics, Daiichi Sankyo, GSK, Lilly, Merck, MyoKardia, Novartis, Roche, Theracos, Quantum Genomics, Cardurion, Janssen, Cardiac Dimensions, Tenaya, Sanofi Pasteur, Dinaqor, Tremeau, CellProthera, Moderna, American Regent, Sarepta, Lexicon, AnaCardio, Akros, and Valo. R.H. reports institutional grants from Abbott, Biotronik, and Slovak Research and Development Agency; honoraria from Abbott and Medtronic; and travel grants from the European Society of Cardiology and Pfizer. He is also the president of the Slovak Heart Rhythm Association. E.M. reports grants from Novartis, Boehringer Ingelheim, and Biotronik Hungary. V.K. reports grants from Boston Scientific, ZOLL, Biotronik, Spire Inc., and NIH, consulting fees from Biotronik and Zoll, and payment or honoraria for lectures from Abbott Medical and Medtronic. The other authors declare no conflict of interest for this contribution.
Figures
References
-
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation 2020;141:e139–596. - PubMed
-
- Lamas GA, Lee KL, Sweeney MO, Silverman R, Leon A, Yee R et al. Ventricular pacing or dual-chamber pacing for sinus-node dysfunction. N Engl J Med 2002;346:1854–62. - PubMed
-
- Wilkoff BL, Cook JR, Epstein AE, Greene HL, Hallstrom AP, Hsia H et al. Dual-chamber pacing or ventricular backup pacing in patients with an implantable defibrillator: the Dual Chamber and VVI Implantable Defibrillator (DAVID) trial. JAMA 2002;288:3115–23. - PubMed
-
- Kiehl EL, Makki T, Kumar R, Gumber D, Kwon DH, Rickard JW et al. Incidence and predictors of right ventricular pacing-induced cardiomyopathy in patients with complete atrioventricular block and preserved left ventricular systolic function. Heart Rhythm 2016;13:2272–8. - PubMed
-
- Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM et al. 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: developed by the task force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) with the special contribution of the European Heart Rhythm Association (EHRA). Eur Heart J 2021;42:3427–520. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
