

Urine output is an early and strong predictor of acute kidney injury and associated mortality: a systematic literature review of 50 clinical studies
- PMID: 38980557
- PMCID: PMC11233478
- DOI: 10.1186/s13613-024-01342-x
Urine output is an early and strong predictor of acute kidney injury and associated mortality: a systematic literature review of 50 clinical studies
Abstract
Background: Although the present diagnosis of acute kidney injury (AKI) involves measurement of acute increases in serum creatinine (SC) and reduced urine output (UO), measurement of UO is underutilized for diagnosis of AKI in clinical practice. The purpose of this investigation was to conduct a systematic literature review of published studies that evaluate both UO and SC in the detection of AKI to better understand incidence, healthcare resource use, and mortality in relation to these diagnostic measures and how these outcomes may vary by population subtype.
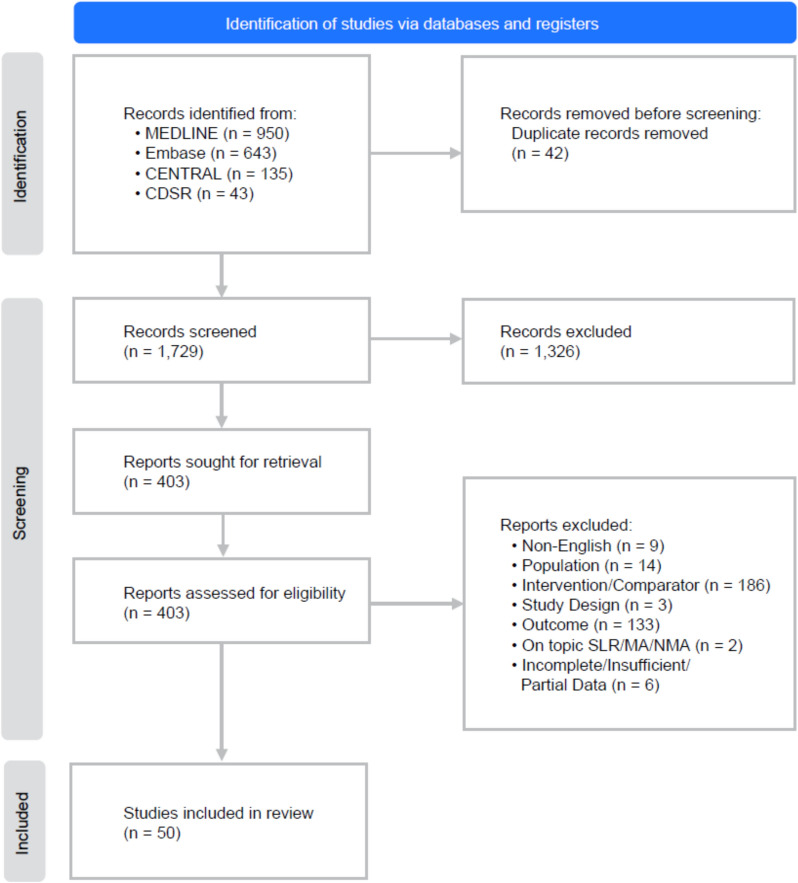
Methods: The systematic literature review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. Data were extracted from comparative studies focused on the diagnostic accuracy of UO and SC, relevant clinical outcomes, and resource usage. Quality and validity were assessed using the National Institute for Health and Care Excellence (NICE) single technology appraisal quality checklist for randomized controlled trials and the Newcastle-Ottawa Quality Assessment Scale for observational studies.
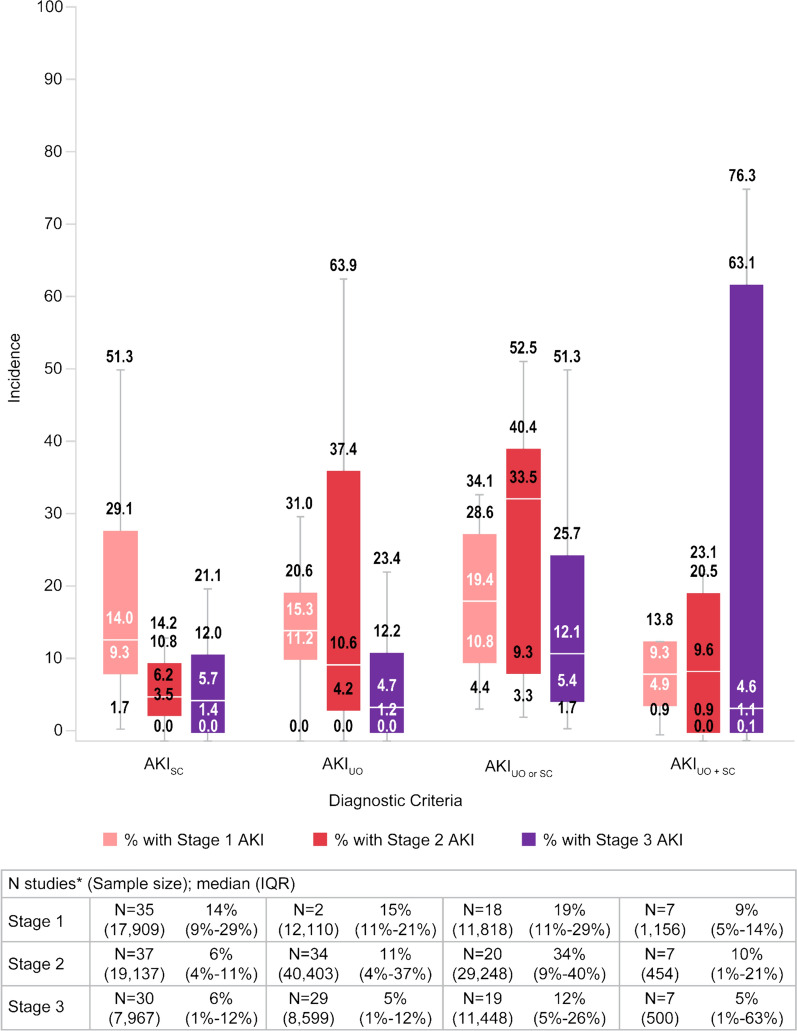
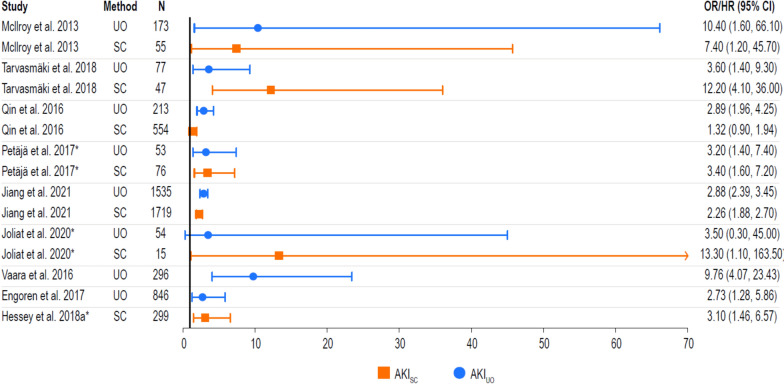
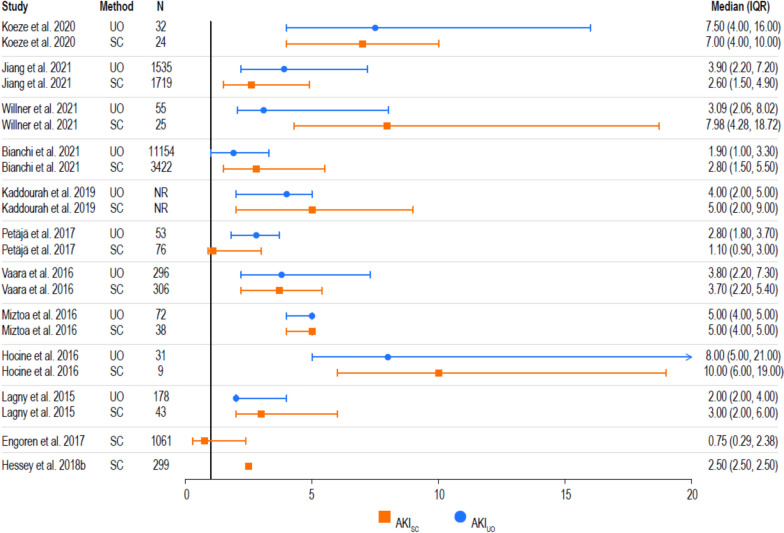
Results: A total of 1729 publications were screened, with 50 studies eligible for inclusion. A majority of studies (76%) used the Kidney Disease: Improving Global Outcomes (KDIGO) criteria to classify AKI and focused on the comparison of UO alone versus SC alone, while few studies analyzed a diagnosis of AKI based on the presence of both UO and SC, or the presence of at least one of UO or SC indicators. Of the included studies, 33% analyzed patients treated for cardiovascular diseases and 30% analyzed patients treated in a general intensive care unit. The use of UO criteria was more often associated with increased incidence of AKI (36%), than was the application of SC criteria (21%), which was consistent across the subgroup analyses performed. Furthermore, the use of UO criteria was associated with an earlier diagnosis of AKI (2.4-46.0 h). Both diagnostic modalities accurately predicted risk of AKI-related mortality.
Conclusions: Evidence suggests that the inclusion of UO criteria provides substantial diagnostic and prognostic value to the detection of AKI.
Keywords: AKIN; Acute kidney injury; Detection; Epidemiology; KDIGO; Prognosis; RIFLE; Serum creatinine; Systematic literature review; Urine output.
© 2024. The Author(s).
Conflict of interest statement
MLNGM is Professor of Critical Care Research at the First Department of Anesthesiology and Intensive Therapy, Medical University of Lublin, Poland. He is co-founder, past-President, and current Treasurer of WSACS (The Abdominal Compartment Society,
Figures


Similar articles
-
Early identification of acute kidney injury in the ICU with real-time urine output monitoring: a clinical investigation.BMC Nephrol. 2021 Aug 26;22(1):293. doi: 10.1186/s12882-021-02485-w. BMC Nephrol. 2021. PMID: 34445954 Free PMC article.
-
Definition of hourly urine output influences reported incidence and staging of acute kidney injury.BMC Nephrol. 2020 Jan 15;21(1):19. doi: 10.1186/s12882-019-1678-2. BMC Nephrol. 2020. PMID: 31941447 Free PMC article.
-
Prognostic implications of adding urine output to serum creatinine measurements for staging of acute kidney injury after major surgery: a cohort study.Nephrol Dial Transplant. 2016 Dec;31(12):2049-2056. doi: 10.1093/ndt/gfw374. Nephrol Dial Transplant. 2016. PMID: 27941063
-
Incidence, timing and outcome of AKI in critically ill patients varies with the definition used and the addition of urine output criteria.BMC Nephrol. 2017 Feb 20;18(1):70. doi: 10.1186/s12882-017-0487-8. BMC Nephrol. 2017. PMID: 28219327 Free PMC article. Review.
-
Acute Kidney Injury: Diagnosis and Classification in Adults and Children.Contrib Nephrol. 2018;193:1-12. doi: 10.1159/000484956. Epub 2018 Jan 23. Contrib Nephrol. 2018. PMID: 29393148 Review.
Cited by
-
Machine learning-derived multivariate renal function trajectories in acute kidney injury in critically ill patients: a multicentre retrospective study.Clin Kidney J. 2025 May 6;18(6):sfaf142. doi: 10.1093/ckj/sfaf142. eCollection 2025 Jun. Clin Kidney J. 2025. PMID: 40469838 Free PMC article.
-
Prognostic value of dynamic KDIGO staging in acute kidney injury after acute heart failure: a doubly robust analysis.Sci Rep. 2025 Jul 2;15(1):22920. doi: 10.1038/s41598-025-07118-y. Sci Rep. 2025. PMID: 40594651 Free PMC article.
-
Impact of prognostic scores on acute kidney injury assessment in the postoperative period of myocardial revascularization.Rev Esc Enferm USP. 2025 Apr 14;59:e20240410. doi: 10.1590/1980-220X-REEUSP-2024-0410en. eCollection 2025. Rev Esc Enferm USP. 2025. PMID: 40233209 Free PMC article.
References
-
- Shinjo H, Sato W, Imai E, Kosugi T, Hayashi H, Nishimura K, Nishiwaki K, Yuzawa Y, Matsuo S, Maruyama S. Comparison of kidney disease: improving global outcomes and acute kidney injury network criteria for assessing patients in intensive care units. Clin Exp Nephrol. 2014;18(5):737–745. doi: 10.1007/s10157-013-0915-4. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
