

Internet-Guided Cognitive Behavioral Therapy for Insomnia Among Patients With Traumatic Brain Injury: A Randomized Clinical Trial
- PMID: 38980675
- PMCID: PMC11234237
- DOI: 10.1001/jamanetworkopen.2024.20090
Internet-Guided Cognitive Behavioral Therapy for Insomnia Among Patients With Traumatic Brain Injury: A Randomized Clinical Trial
Abstract
Importance: Many military service members and veterans report insomnia after sustaining traumatic brain injury (TBI). Limitations of first-line treatment, cognitive-behavioral therapy for insomnia (CBT-I), include availability of qualified clinicians, low completion rates, and cost.
Objective: To investigate the feasibility and efficacy of internet-guided CBT-I (eCBT-I) in military service members and veterans with insomnia and a history of TBI.
Design, setting, and participants: This randomized clinical trial of fully remote internet-based interventions and evaluations was conducted from September 1, 2020, to June 30, 2021, with 3 months of follow-up. Participants included a volunteer sample of military service members and veterans aged 18 to 64 years with a history of mild TBI/concussion and at least moderately severe insomnia defined as an insomnia severity index (ISI) score of greater than 14 and Pittsburgh Sleep Quality Index of greater than 4. Self-reported race, ethnicity, and educational level were generally representative of the US military. Data were analyzed from October 21, 2021, to April 29, 2024.
Intervention: Internet-based CBT-I delivered over 6 weekly lesson modules with assigned homework activities.
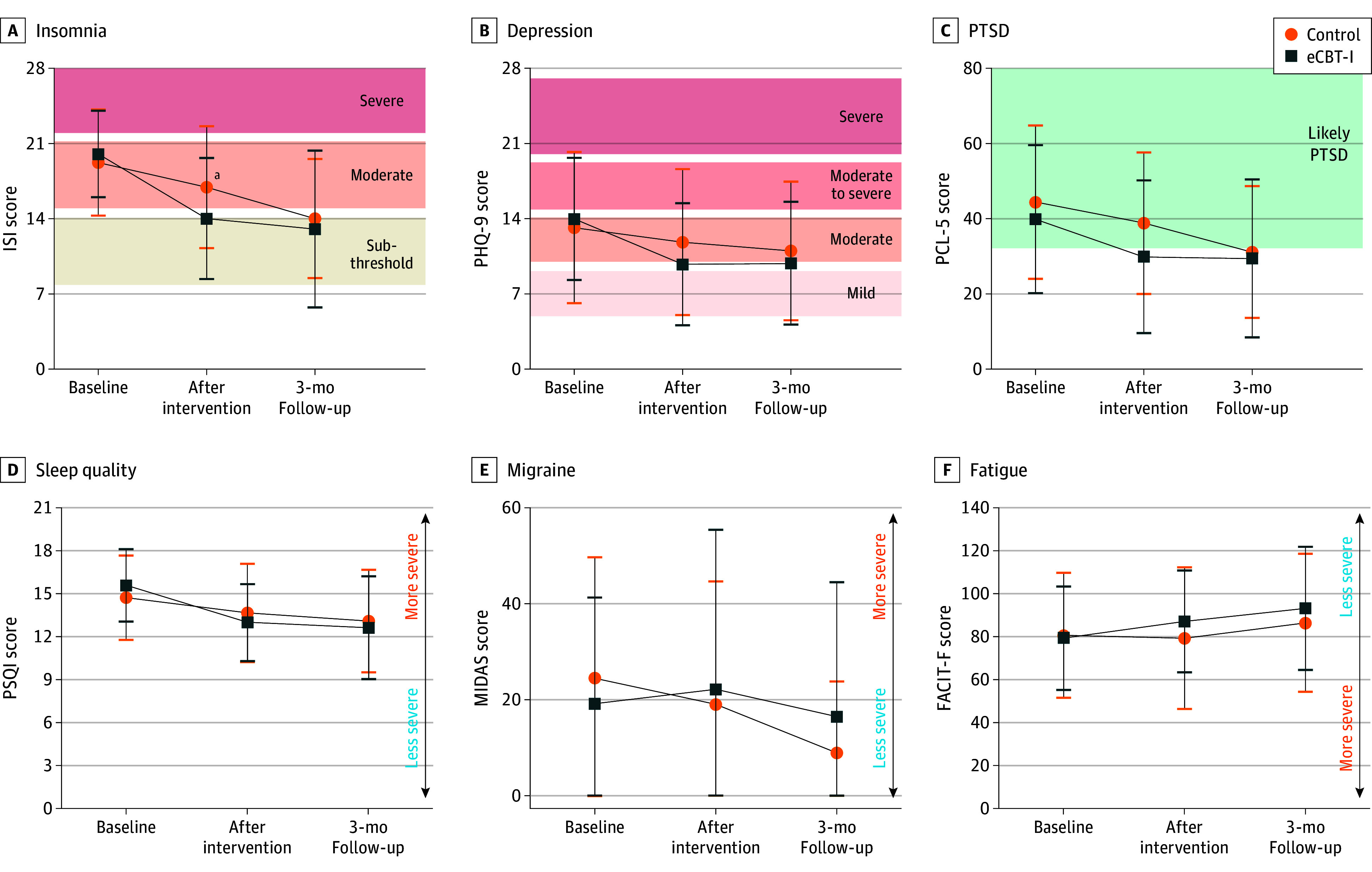
Main outcomes and measures: The prespecified primary outcome measure was change in ISI score over time. Prespecified secondary outcome measures included self-reported measures of depression symptoms, posttraumatic stress disorder (PTSD) symptoms, sleep quality, migraine impact, and fatigue.
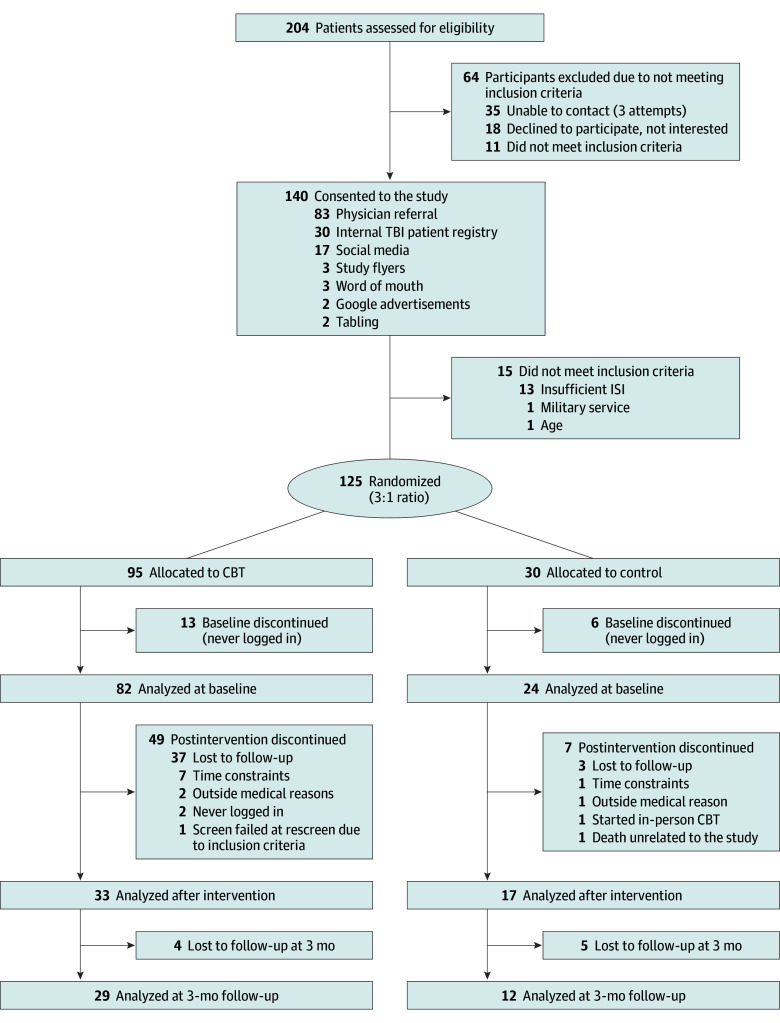
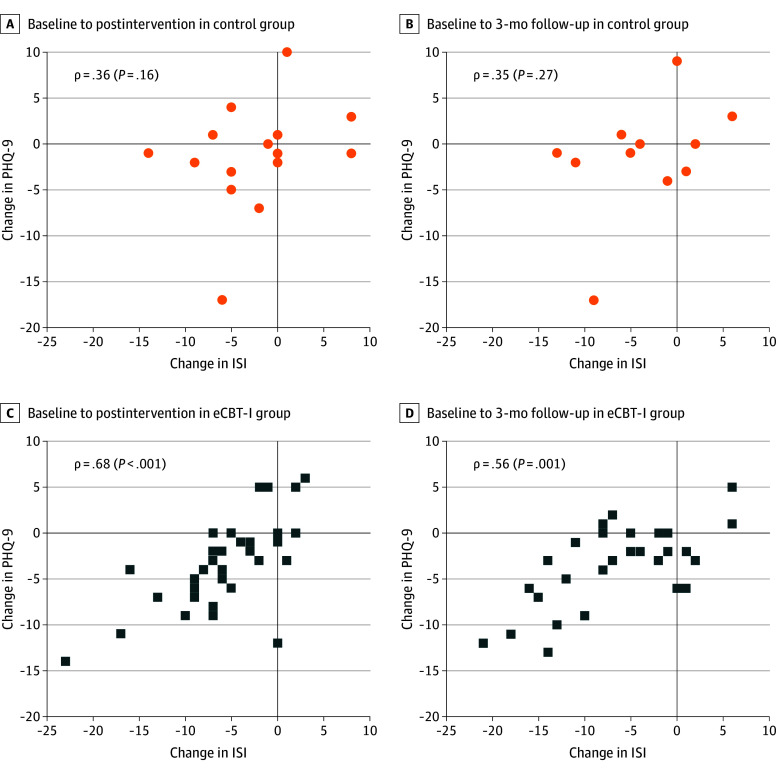
Results: Of 204 people screened, 125 were randomized 3:1 to eCBT-I vs online sleep education, and 106 completed baseline evaluations (83 men [78.3%]; mean [SD] age, 42 [12] years). Of these, 22 participants (20.8%) were Hispanic or Latino and 78 (73.6%) were White. Fifty participants completed postintervention evaluations, and 41 completed the 3-month follow-up. Baseline mean (SD) ISI scores were 19.7 (4.0) in those randomized to eCBT-I and 18.9 (5.0) in those randomized to sleep education. After intervention, mean (SD) ISI scores were 13.7 (5.6) in those randomized to eCBT-I and 16.6 (5.7) in those randomized to sleep education. The difference in the extent of reduction in ISI scores between groups was 3.5 (95% CI,-6.5 to -0.4 [P = .03]; Cohen d, -0.32 [95% CI, -0.70 to -0.04]). In the eCBT-I group, the extent of insomnia improvement correlated with the extent of depressive symptom improvement (Spearman ρ = 0.68 [P < .001]), PTSD symptoms (ρ = 0.36 [P = .04]), sleep quality (ρ = 0.54 [P = .001]), and fatigue impact (ρ = -0.58 [P < .001]) but not migraine-related disability.
Conclusions and relevance: The findings of this randomized clinical trial suggest that fully remote eCBT-I was moderately feasible and effective for self-reported insomnia and depression symptoms in military service members and veterans with a history of TBI. There is great potential benefit for eCBT-I due to low availability and cost of qualified CBT-I clinicians, although optimization of completion rates remains a challenge. Future studies may use home-based objective sleep assessments and should increase study retention.
Trial registration: ClinicalTrials.gov Identifier: NCT04377009.
Conflict of interest statement
Figures
References
-
- Health.mil . DOD TBI worldwide numbers. Accessed June 12, 2023. http://health.mil/Military-Health-Topics/Centers-of-Excellence/Traumatic...
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
