

Inflammatory bowel disease associated with primary sclerosing cholangitis is associated with an altered gut microbiome and bile acid profile
- PMID: 38980940
- PMCID: PMC11637524
- DOI: 10.1093/ecco-jcc/jjae096
Inflammatory bowel disease associated with primary sclerosing cholangitis is associated with an altered gut microbiome and bile acid profile
Abstract
Background: Primary sclerosing cholangitis associated with inflammatory bowel disease (IBD-PSC) carries significant morbidity compared to IBD without PSC. Alterations in microbial composition and bile acid (BA) profiles have been shown to modulate chronic inflammation in IBD, but data in IBD-PSC is scarce. We aimed to assess the differences in gut microbiome composition as well as in the BA profile and BA-related microbial functions between IBD-PSC and IBD-only.
Methods: 54 IBD-PSC and 62 IBD-only subjects were enrolled from 2012 to 2021. Baseline samples were collected for fecal DNA shotgun metagenomic sequencing, fecal and serum BA quantitation using mass spectrometry and fecal calprotectin. Liver fibrosis measured by transient elastography (TE) was assessed in the IBD-PSC group. Data was analyzed using general linear regression models and Spearman rank correlation tests.
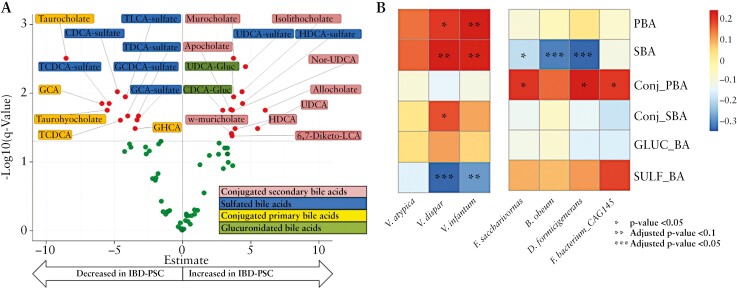
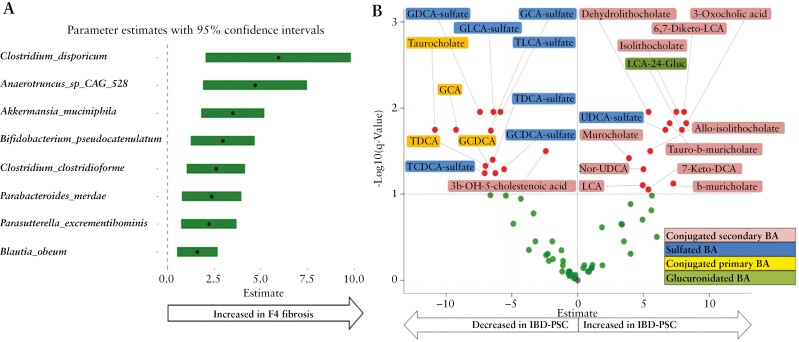
Results: Patients with IBD-PSC had reduced microbial gene richness (p=0.004) and significant compositional shifts (PERMANOVA: R2=0.01, p=0.03) compared to IBD-only. IBD-PSC was associated with altered microbial composition and function, including decreased abundance of Blautia obeum, increased abundance of Veillonella atypica, Veillonella dispar and Clostridium scindens (q<0.05 for all), and increased abundance of microbial genes involved in secondary BA metabolism. Decreased serum sulfated and increased serum conjugated secondary BA were associated with IBD-PSC and increased liver fibrosis.
Conclusion: We identified differences in microbial species, functional capacity and serum BA profiles in IBD-PSC compared with IBD-only. Our findings provide insight into the pathophysiology of IBD associated with PSC and suggest possible targets for modulating the risk and course of IBD in subjects with PSC.
Keywords: Bile acids; Gut microbiome; Inflammatory Bowel Disease; Primary Sclerosing Cholangitis.
© The Author(s) 2024. Published by Oxford University Press on behalf of European Crohn’s and Colitis Organisation.
Conflict of interest statement
All authors disclose no potential conflicts [financial, professional, or personal] that are relevant to the manuscript.
Figures


References
-
- Karlsen TH, Folseraas T, Thorburn D, Vesterhus M.. Primary sclerosing cholangitis – a comprehensive review. J Hepatol 2017;67:1298–323. - PubMed
-
- Kummen M, Holm K, Anmarkrud JA, et al. The gut microbial profile in patients with primary sclerosing cholangitis is distinct from patients with ulcerative colitis without biliary disease and healthy controls. Gut 2017;66:611–9. - PubMed
LinkOut - more resources
Full Text Sources
