

Identification of Parkinson's disease PACE subtypes and repurposing treatments through integrative analyses of multimodal data
- PMID: 38982243
- PMCID: PMC11233682
- DOI: 10.1038/s41746-024-01175-9
Identification of Parkinson's disease PACE subtypes and repurposing treatments through integrative analyses of multimodal data
Abstract
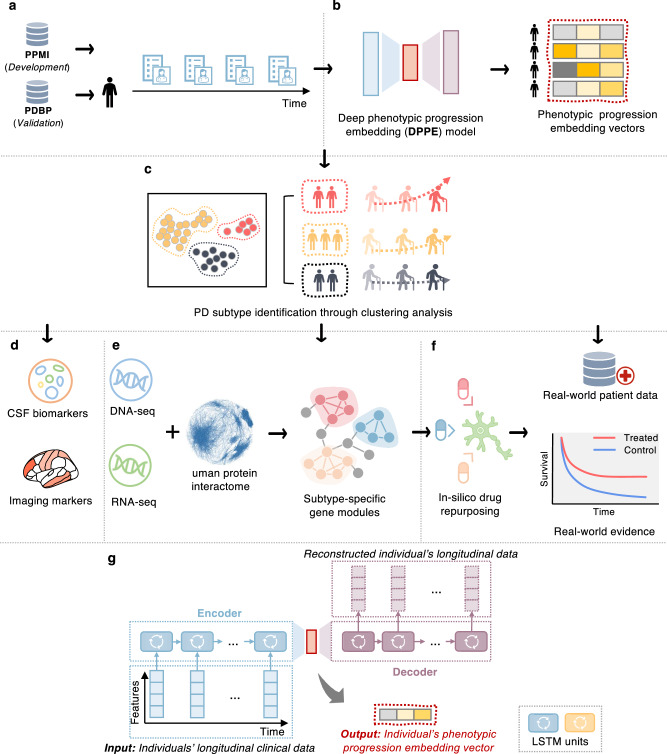
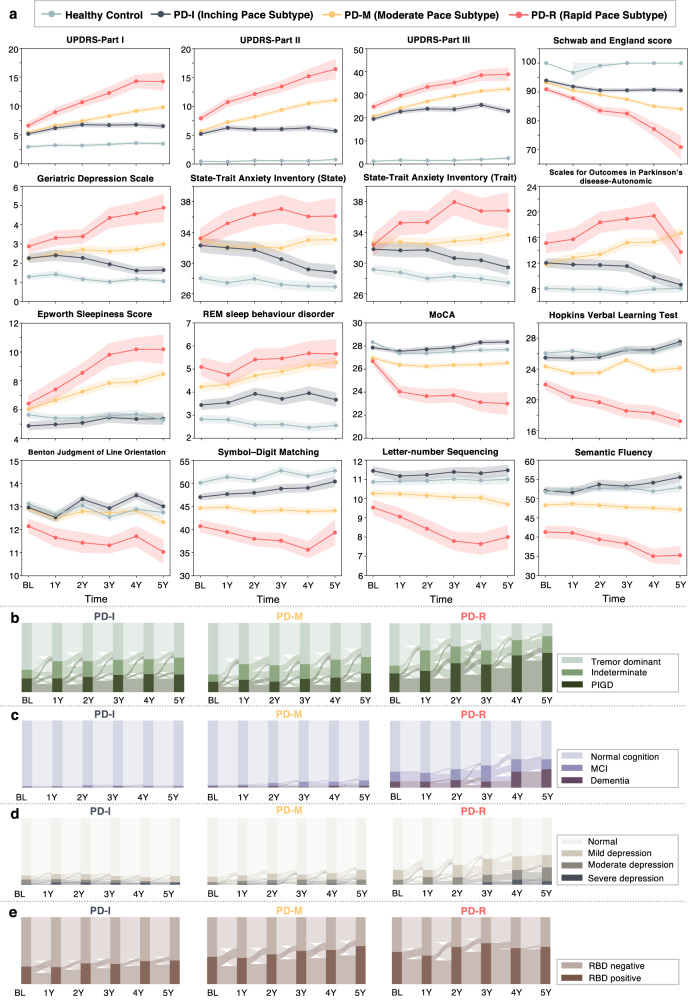
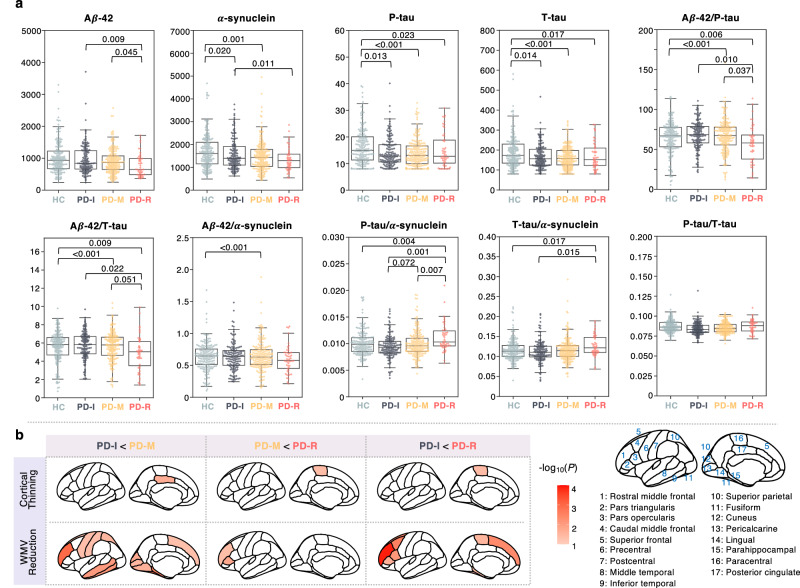
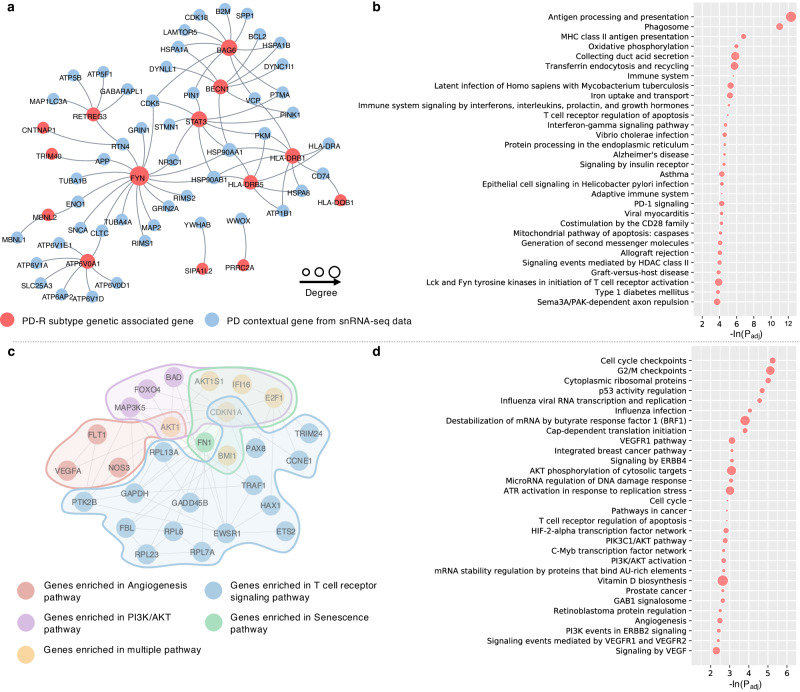
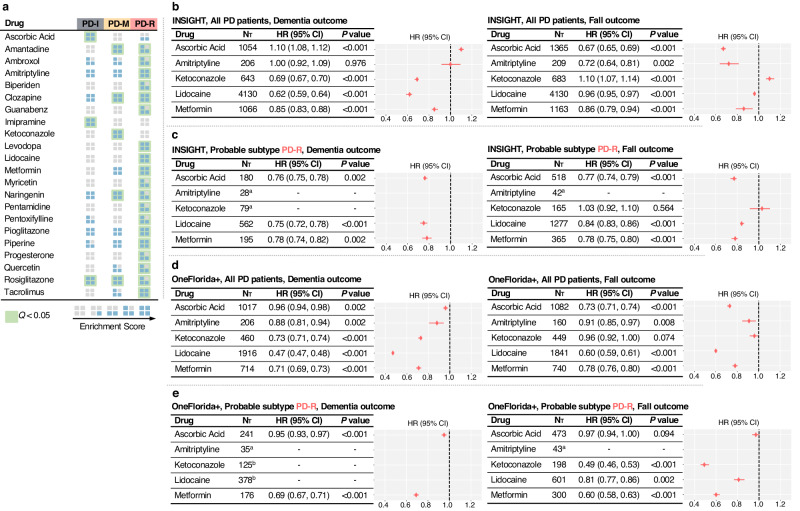
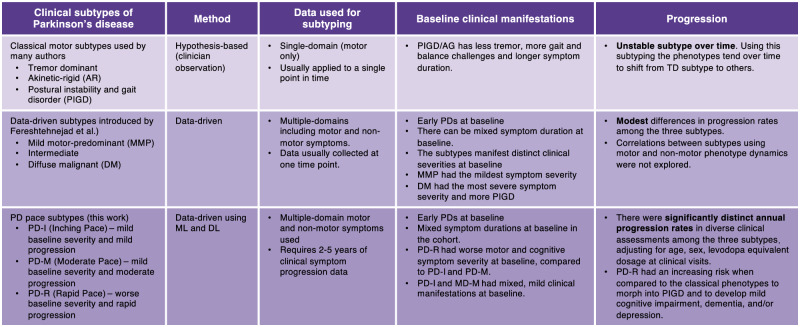
Parkinson's disease (PD) is a serious neurodegenerative disorder marked by significant clinical and progression heterogeneity. This study aimed at addressing heterogeneity of PD through integrative analysis of various data modalities. We analyzed clinical progression data (≥5 years) of individuals with de novo PD using machine learning and deep learning, to characterize individuals' phenotypic progression trajectories for PD subtyping. We discovered three pace subtypes of PD exhibiting distinct progression patterns: the Inching Pace subtype (PD-I) with mild baseline severity and mild progression speed; the Moderate Pace subtype (PD-M) with mild baseline severity but advancing at a moderate progression rate; and the Rapid Pace subtype (PD-R) with the most rapid symptom progression rate. We found cerebrospinal fluid P-tau/α-synuclein ratio and atrophy in certain brain regions as potential markers of these subtypes. Analyses of genetic and transcriptomic profiles with network-based approaches identified molecular modules associated with each subtype. For instance, the PD-R-specific module suggested STAT3, FYN, BECN1, APOA1, NEDD4, and GATA2 as potential driver genes of PD-R. It also suggested neuroinflammation, oxidative stress, metabolism, PI3K/AKT, and angiogenesis pathways as potential drivers for rapid PD progression (i.e., PD-R). Moreover, we identified repurposable drug candidates by targeting these subtype-specific molecular modules using network-based approach and cell line drug-gene signature data. We further estimated their treatment effects using two large-scale real-world patient databases; the real-world evidence we gained highlighted the potential of metformin in ameliorating PD progression. In conclusion, this work helps better understand clinical and pathophysiological complexity of PD progression and accelerate precision medicine.
© 2024. The Author(s).
Conflict of interest statement
J.C. has provided consultation to Acadia, Actinogen, Acumen, AlphaCognition, ALZpath, Aprinoia, AriBio, Artery, Biogen, Biohaven, BioVie, BioXcel, Bristol-Myers Squib, Cassava, Cerecin, Diadem, Eisai, GAP Foundation, GemVax, Janssen, Jocasta, Karuna, Lighthouse, Lilly, Lundbeck, LSP/eqt, Merck, NervGen, New Amsterdam, Novo Nordisk, Oligomerix, Optoceutics, Ono, Otsuka, Oxford Brain Diagnostics, Prothena, ReMYND, Roche, Sage Therapeutics, Signant Health, Simcere, sinaptica, Suven, TrueBinding, Vaxxinity, and Wren pharmaceutical, assessment, and investment companies. The other authors declare no Competing Financial or Non-Financial Interests.
Figures
References
-
- Mizuno Y. Where do we stand in the treatment of Parkinson’s disease? J. Neurol. 2007;254:13–18. doi: 10.1007/s00415-007-5003-9. - DOI
Grants and funding
- R21 AG083003/AG/NIA NIH HHS/United States
- R01 AG082118/AG/NIA NIH HHS/United States
- R56 AG074001/AG/NIA NIH HHS/United States
- R01AG076448/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- RF1AG072449/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- MJFF-023081/Michael J. Fox Foundation for Parkinson's Research (Michael J. Fox Foundation)
- R01AG080991/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- P30 AG072959/AG/NIA NIH HHS/United States
- 3R01AG066707-01S1/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- R21AG083003/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- R01AG066707/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- R35 AG071476/AG/NIA NIH HHS/United States
- RF1 AG082211/AG/NIA NIH HHS/United States
- R56AG074001/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- R01AG082118/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- R25 AG083721/AG/NIA NIH HHS/United States
- RF1AG082211/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- U01 NS093334/NS/NINDS NIH HHS/United States
- AG083721-01/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- RF1NS133812/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- P20GM109025/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- RF1 NS133812/NS/NINDS NIH HHS/United States
- R35AG71476/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- U01 AG073323/AG/NIA NIH HHS/United States
- R01 AG066707/AG/NIA NIH HHS/United States
- R01AG053798/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- R01AG076234/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- R01 AG076448/AG/NIA NIH HHS/United States
- R01 AG080991/AG/NIA NIH HHS/United States
- R01 AG076234/AG/NIA NIH HHS/United States
- U01NS093334/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- P20 GM109025/GM/NIGMS NIH HHS/United States
- P30AG072959/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- RF1 AG072449/AG/NIA NIH HHS/United States
- R01 AG053798/AG/NIA NIH HHS/United States
- 3R01AG066707-02S1/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- U01AG073323/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- ALZDISCOVERY-1051936/ALZ/Alzheimer's Association/United States
LinkOut - more resources
Full Text Sources
Miscellaneous
