

Physiological and clinical effects of trunk inclination adjustment in patients with respiratory failure: a scoping review and narrative synthesis
- PMID: 38982466
- PMCID: PMC11232125
- DOI: 10.1186/s13054-024-05010-1
Physiological and clinical effects of trunk inclination adjustment in patients with respiratory failure: a scoping review and narrative synthesis
Abstract
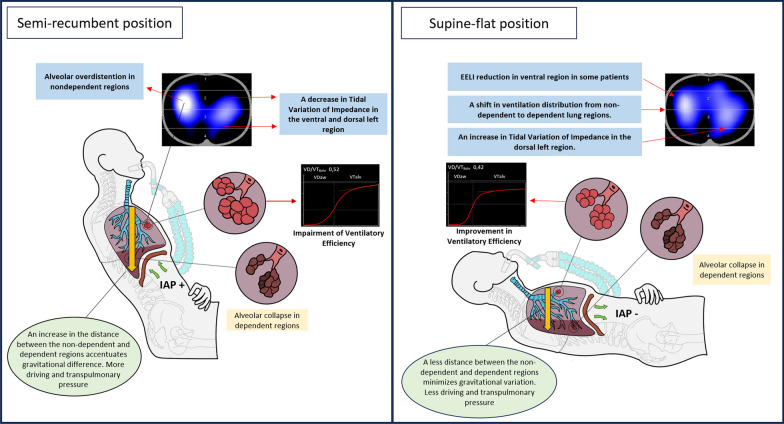
Background: Adjusting trunk inclination from a semi-recumbent position to a supine-flat position or vice versa in patients with respiratory failure significantly affects numerous aspects of respiratory physiology including respiratory mechanics, oxygenation, end-expiratory lung volume, and ventilatory efficiency. Despite these observed effects, the current clinical evidence regarding this positioning manoeuvre is limited. This study undertakes a scoping review of patients with respiratory failure undergoing mechanical ventilation to assess the effect of trunk inclination on physiological lung parameters.
Methods: The PubMed, Cochrane, and Scopus databases were systematically searched from 2003 to 2023.
Interventions: Changes in trunk inclination.
Measurements: Four domains were evaluated in this study: 1) respiratory mechanics, 2) ventilation distribution, 3) oxygenation, and 4) ventilatory efficiency.
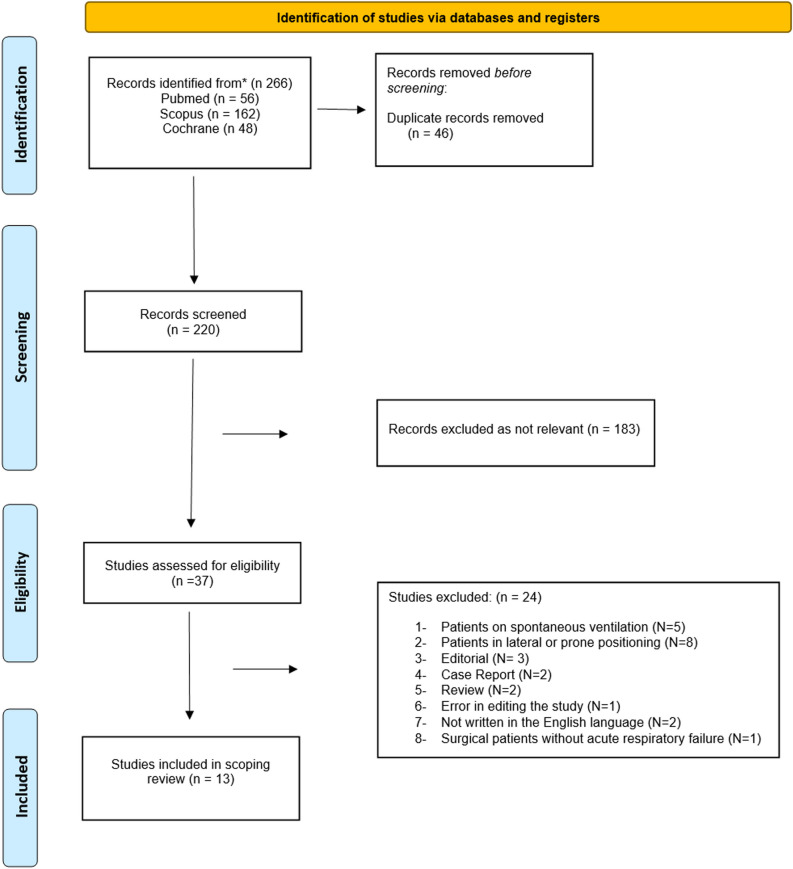
Results: After searching the three databases and removing duplicates, 220 studies were screened. Of these, 37 were assessed in detail, and 13 were included in the final analysis, comprising 274 patients. All selected studies were experimental, and assessed respiratory mechanics, ventilation distribution, oxygenation, and ventilatory efficiency, primarily within 60 min post postural change.
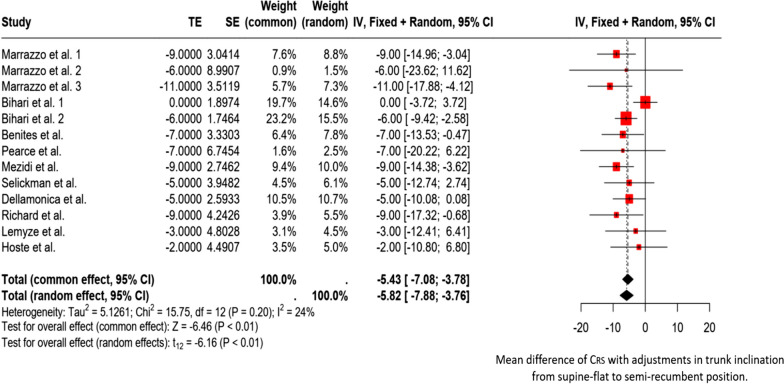
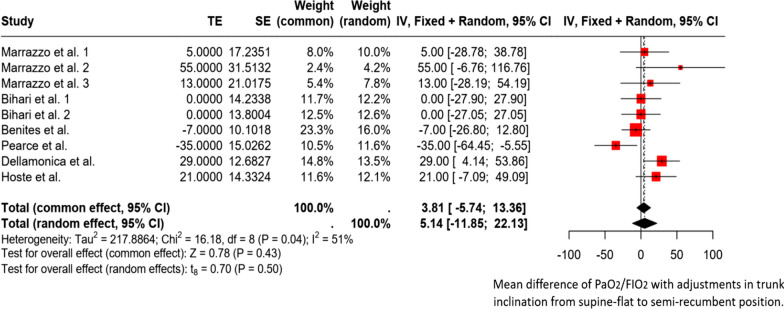
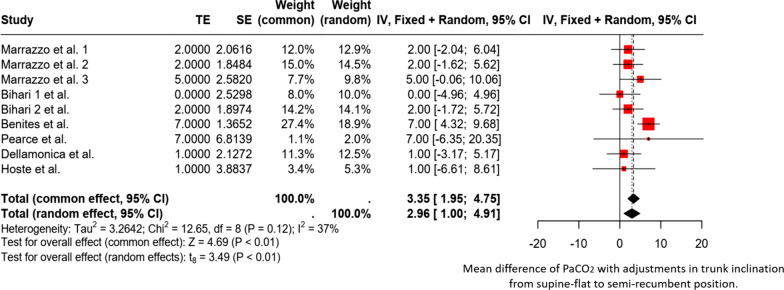
Conclusion: In patients with acute respiratory failure, transitioning from a supine to a semi-recumbent position leads to decreased respiratory system compliance and increased airway driving pressure. Additionally, C-ARDS patients experienced an improvement in ventilatory efficiency, which resulted in lower PaCO2 levels. Improvements in oxygenation were observed in a few patients and only in those who exhibited an increase in EELV upon moving to a semi-recumbent position. Therefore, the trunk inclination angle must be accurately reported in patients with respiratory failure under mechanical ventilation.
Keywords: Acute respiratory distress syndrome; Body position; Driving pressure; End-expiratory lung volume; Respiratory dead space; Tidal volume; Trunk inclination.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests. Additional file 1: Expert panel, Search string, characteristics tables of the studies, review-specifc risk of bias rating guidance, supplementary tables. Additional file 2: Risk of bias.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
