

A case of IgG4-related disease manifesting as a spinal epidural mass
- PMID: 38983111
- PMCID: PMC11233069
- DOI: 10.1093/bjrcr/uaae022
A case of IgG4-related disease manifesting as a spinal epidural mass
Abstract
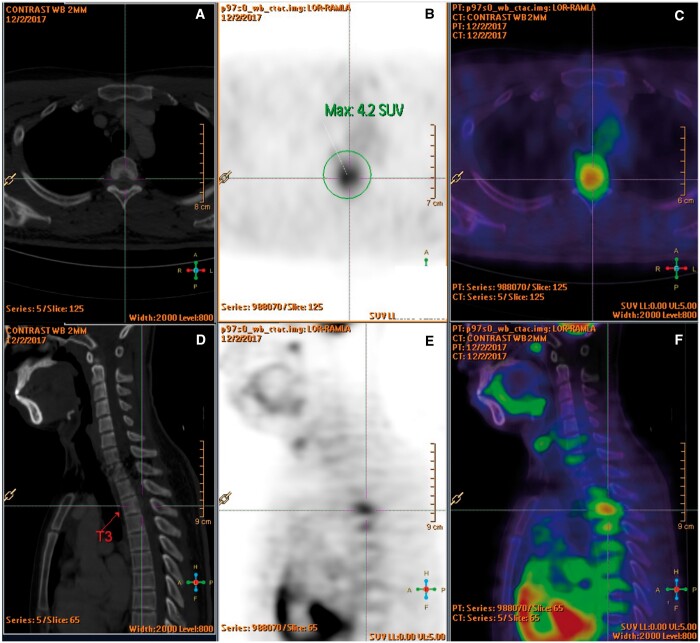
IgG4-related disease is an immune-mediated fibroinflammatory condition. Isolated manifestation in the spine as hypertrophic pachymeningitis is very rare and the mass-like lesion on MRI often mimic tumour or infection. Patients would present with symptoms that result from mass effect or neurovascular compression. Studies showed that serum and CSF IgG4 levels are rarely informative, and therefore, tissue biopsy is crucial for accurate diagnosis. Apart from supporting the diagnosis, MRI is helpful in delineating the extent of disease and follow-up after treatment. A 18F-FDG PET/CT scan is useful in detecting systemic manifestations of IgG4-related disease. Although IgG4-related disease generally responds well to corticosteroid at inflammatory state, relapse is not uncommon. Current treatment strategies for IgG4-related hypertrophic pachymeningitis are high dose corticosteroid therapy and early decompressive surgery to avoid chronic neurological complications. We described a case of a 27-year-old gentleman complaining of lower limb weakness and numbness. MRI showed a mass-like epidural lesion at the thoracic spine causing cord compression. Open biopsy of the epidural mass demonstrated histopathological characteristics of IgG4-related disease. Patient responded well to early surgical decompression of the spinal cord and corticosteroid as evidenced by symptom improvement and resolving mass on subsequent MRI study. However, a follow-up MRI revealed disease recurrence years later.
Keywords: IgG4; IgG4-related disease; IgG4-related hypertrophic pachymeningitis; MRI; epidural mass; hypertrophic pachymeningitis.
© The Author(s) 2024. Published by Oxford University Press on behalf of the British Institute of Radiology.
Conflict of interest statement
The authors have no conflicts of interest.
Figures



References
-
- Umehara H, Okazaki K, Kawa S, et al.Research Program for Intractable Disease by the Ministry of Health, Labor and Welfare (MHLW) Japan. The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD. Mod Rheumatol. 2021;31(3):529-533. - PubMed
-
- Chan SK, Cheuk W, Chan KT, Chan JK.. IgG4-related sclerosing pachymeningitis: a previously unrecognized form of central nervous system involvement in IgG4-related sclerosing disease. Am J Surg Pathol. 2009;33(8):1249-1252. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
