

Thoracoscopic pulmonary resection combined with real-time image-guided percutaneous ablation for multiple pulmonary nodules: a novel surgical approach and literature review
- PMID: 38983149
- PMCID: PMC11228749
- DOI: 10.21037/jtd-23-1986
Thoracoscopic pulmonary resection combined with real-time image-guided percutaneous ablation for multiple pulmonary nodules: a novel surgical approach and literature review
Abstract
Background: Due to the widespread use of computed tomography (CT) screening and advances in diagnostic techniques, an increasing number of patients with multiple pulmonary nodules are being detected and pathologically diagnosed as synchronous multiple primary lung cancers (sMPLC). It has become a new challenge to treat multiple pulmonary nodules and obtain a favorable prognosis while minimizing the perioperative risk for patients. The purpose of this study was to summarize the preliminary experience with a hybrid surgery combining pulmonary resection and ablation for the treatment of sMPLC and to discuss the feasibility of this novel procedure with a literature review.
Methods: This is a retrospective non-randomized controlled study. From January 1, 2022 to July 1, 2023, four patients underwent hybrid surgery combining thoracoscopic pulmonary resection and percutaneous pulmonary ablation for multiple pulmonary nodules. Patients were followed up at 3, 6 and 12 months postoperatively and the last follow-up was on November 30, 2023. Clinical characteristics, perioperative outcomes, pulmonary function recovery and oncologic prognosis were recorded. Meanwhile we did a literature review of studies on hybridized pulmonary surgery for the treatment of multiple pulmonary nodules.
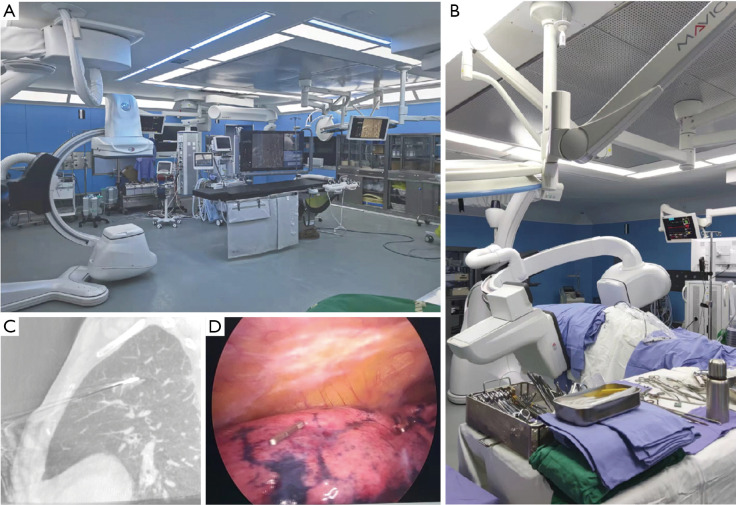
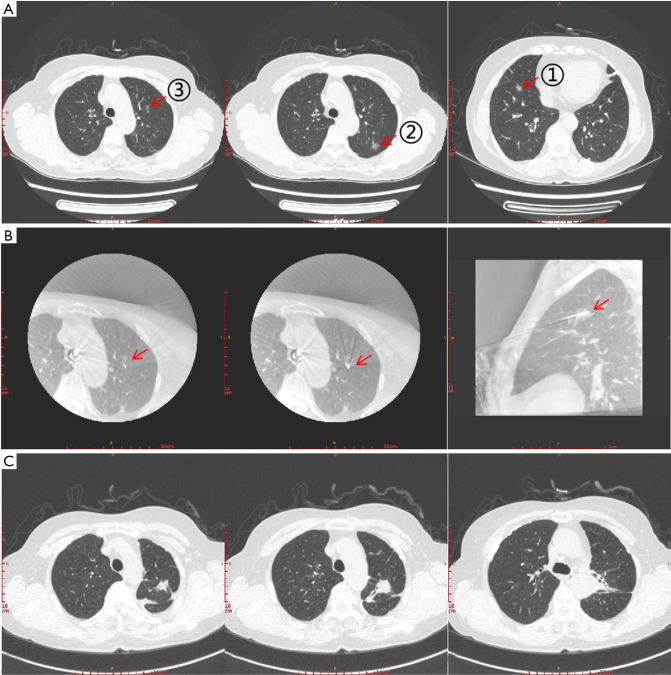
Results: All the four patients were female, aged 52 to 70 years, and had no severe cardiopulmonary dysfunction on preoperative examination. Hybrid surgery of simultaneous pulmonary resection and ablation were performed in these patients to treat 2 to 4 pulmonary nodules, assisted by intraoperative real-time guide of C-arm X-ray machine. The operation time was from 155 to 240 minutes, and intraoperative blood loss was from 50 to 200 mL. Postoperative hospital stay was 2 to 7 days, thoracic drainage duration was 2 to 6 days, and pleural drainage volume was 300-1,770 mL. One patient presented with a bronchopleural fistula due to pulmonary ablation; the fistula was identified and sutured during thoracoscopic surgery and the patient recovered well. No postoperative 90-day complications occurred. After 3 months postoperatively, performance status scores for these patients recovered to 80 to 100. No tumor recurrence or metastasis was detected during the follow-up period.
Conclusions: Hybrid procedures combining minimally invasive pulmonary resection with ablation are particularly suitable for the simultaneous treatment of sMPLC. Patients had less loss of pulmonary function, fewer perioperative complications, and favorable oncologic prognosis. Hybrid surgery is expected to be a better treatment option for patients with sMPLC.
Keywords: Synchronous multiple primary lung cancers (sMPLC); hybrid surgery; novel surgical strategy; percutaneous microwave ablation.
2024 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-23-1986/coif). All authors report that this study was supported by the National High Level Hospital Clinical Research Funding (No. BJ-2022-185). The authors have no other conflicts of interest to declare.
Figures

References
LinkOut - more resources
Full Text Sources