

Clinical study of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in hypertriglyceridemia-induced acute pancreatitis and acute biliary pancreatitis with persistent organ failure
- PMID: 38983313
- PMCID: PMC11230014
- DOI: 10.4240/wjgs.v16.i6.1647
Clinical study of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in hypertriglyceridemia-induced acute pancreatitis and acute biliary pancreatitis with persistent organ failure
Abstract
Background: The neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) are novel inflammatory indicators that can be used to predict the severity and prognosis of various diseases. We categorize acute pancreatitis by etiology into acute biliary pancreatitis (ABP) and hypertriglyceridemia-induced acute pancreatitis (HTGP).
Aim: To investigate the clinical significance of NLR and PLR in assessing persistent organ failure (POF) in HTGP and ABP.
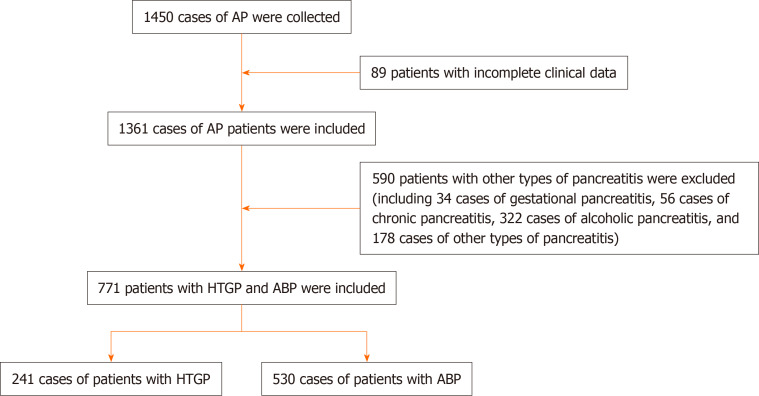
Methods: A total of 1450 patients diagnosed with acute pancreatitis (AP) for the first time at Shanxi Bethune Hospital between January 2012 and January 2023 were enrolled. The patients were categorized into two groups according to the etiology of AP: ABP in 530 patients and HTGP in 241 patients. We collected and compared the clinical data of the patients, including NLR, PLR, and AP prognostic scoring systems, within 48 h of hospital admission.
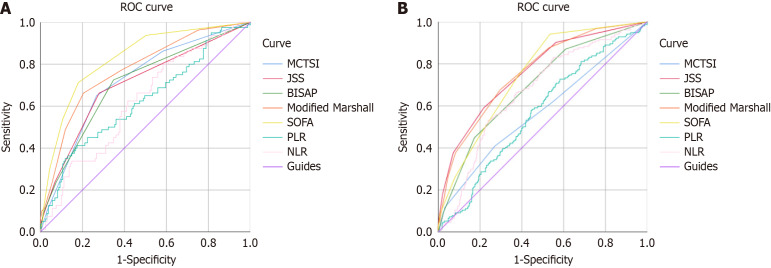
Results: The NLR (9.1 vs 6.9, P < 0.001) and PLR (203.1 vs 160.5, P < 0.001) were significantly higher in the ABP group than in the HTGP group. In the HTGP group, both NLR and PLR were significantly increased in patients with severe AP and those with a SOFA score ≥ 3. Likewise, in the ABP group, NLR and PLR were significantly elevated in patients with severe AP, modified computed tomography severity index score ≥ 4, Japanese Severity Score ≥ 3, and modified Marshall score ≥ 2. Moreover, NLR and PLR showed predictive value for the development of POF in both the ABP and HTGP groups.
Conclusion: NLR and PLR vary between ABP and HTGP, are strongly associated with AP prognostic scoring systems, and have predictive potential for the occurrence of POF in both ABP and HTGP.
Keywords: Acute pancreatitis; Gallstone; Hypertriglyceridemia; Neutrophil-to-lymphocyte ratio; Persistent organ failure; Platelet-to-lymphocyte ratio.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no competing interests.
Figures
Similar articles
-
Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio can predict the severity of gallstone pancreatitis.BMC Gastroenterol. 2018 Jan 25;18(1):18. doi: 10.1186/s12876-018-0748-4. BMC Gastroenterol. 2018. PMID: 29370777 Free PMC article.
-
Evaluation of the prognostic value of neutrophil to lymphocyte ratio in patients with hypertriglyceridemia-induced acute pancreatitis.Pancreatology. 2017 Nov-Dec;17(6):893-897. doi: 10.1016/j.pan.2017.10.001. Epub 2017 Oct 6. Pancreatology. 2017. PMID: 29030078
-
Neutrophil-Lymphocyte Ratio in Patients with Hypertriglyceridemic Pancreatitis Predicts Persistent Organ Failure.Gastroenterol Res Pract. 2022 Mar 16;2022:8333794. doi: 10.1155/2022/8333794. eCollection 2022. Gastroenterol Res Pract. 2022. PMID: 35340692 Free PMC article.
-
Clinical features and treatment of hypertriglyceridemia-induced acute pancreatitis during pregnancy: A retrospective study.J Clin Apher. 2016 Dec;31(6):571-578. doi: 10.1002/jca.21453. Epub 2016 Mar 4. J Clin Apher. 2016. PMID: 26946248
-
Diagnostic utility of hematological indices in predicting adverse outcomes and severity of acute pancreatitis based on BISAP and modified Glasgow score.Ulus Travma Acil Cerrahi Derg. 2022 Mar;28(3):268-275. doi: 10.14744/tjtes.2020.26348. Ulus Travma Acil Cerrahi Derg. 2022. PMID: 35485556 Free PMC article.
References
-
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, Tsiotos GG, Vege SS Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62:102–111. - PubMed
-
- Garcea G, Gouda M, Hebbes C, Ong SL, Neal CP, Dennison AR, Berry DP. Predictors of severity and survival in acute pancreatitis: validation of the efficacy of early warning scores. Pancreas. 2008;37:e54–e61. - PubMed
-
- Johnson CD, Besselink MG, Carter R. Acute pancreatitis. BMJ. 2014;349:g4859. - PubMed
LinkOut - more resources
Full Text Sources
