

Endoscopic radial incision and cutting method for adult congenital duodenal webs: A case report
- PMID: 38983397
- PMCID: PMC11229889
- DOI: 10.12998/wjcc.v12.i18.3622
Endoscopic radial incision and cutting method for adult congenital duodenal webs: A case report
Abstract
Background: Congenital duodenal webs are rare in adults and can lead to various symptoms such as nausea, vomiting, and postprandial fullness. The treatment for this disease is mostly surgical. Endoscopic treatment techniques have been developed and attempted for this disease. Endoscopic radial incision and cutting (RIC) techniques are reportedly very effective in benign anastomotic stricture. This case report highlights the effectiveness and safety of endoscopic RIC as a minimally invasive treatment for adult congenital duodenal webs.
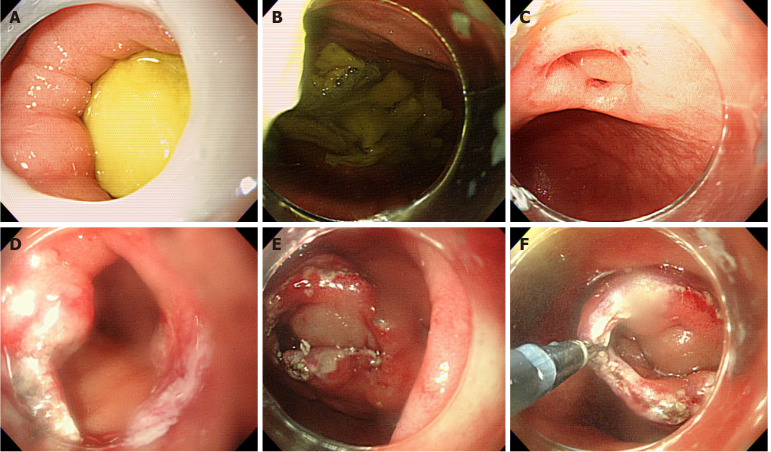
Case summary: A 23-year-old female patient with indigestion was referred to a tertiary hospital. The patient complained of postprandial fullness in the epigastric region. Previous physical examinations or blood tests indicated no abnormalities. Computed tomography revealed an eccentric broad-based delayed-enhancing mass-like lesion in the second portion of the duodenum. Endoscopy showed an enlarged gastric cavity and a significantly dilated duodenal bulb; a very small hole was observed in the distal part of the second portion, and scope passage was not possible. Gastrografin upper gastrointestinal series was performed, revealing an intraduodenal barium contrast-filled sac with a curvilinear narrow radiolucent rim, a typical "windsock" sign. Endoscopic RIC was performed on the duodenal web. The patient recovered uneventfully. Follow-up endoscopy showed a patent duodenal lumen without any residual stenosis. The patient reported complete resolution of symptoms at the 18-month follow-up.
Conclusion: Endoscopic RIC may be an effective treatment for congenital duodenal webs in adults.
Keywords: Case report; Congenital duodenal web; Endoscopic treatment; Radial incision and cutting method; Surgery.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The author reports no relevant conflicts of interest for this article.
Figures




References
-
- Ladd AP, Madura JA. Congenital duodenal anomalies in the adult. Arch Surg. 2001;136:576–584. - PubMed
-
- Alghannam R, Yousef YA. Delayed presentation of a duodenal web. J Pediatr Surg Case Rep. 2015;3:530–533.
-
- Morris G, Kennedy A Jr, Cochran W. Small Bowel Congenital Anomalies: a Review and Update. Curr Gastroenterol Rep. 2016;18:16. - PubMed
-
- Marwah S, Gurawalia JP, Sagu R, Marwah N. Congenital duodenal diaphragm in an adult masquerading as superior mesenteric artery syndrome. Clin J Gastroenterol. 2013;6:217–220. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
