

Outcomes of direct oral anticoagulants with aspirin vs warfarin with aspirin: a registry-based cohort study
- PMID: 38983902
- PMCID: PMC11231707
- DOI: 10.1016/j.rpth.2024.102449
Outcomes of direct oral anticoagulants with aspirin vs warfarin with aspirin: a registry-based cohort study
Abstract
Background: For patients anticoagulated with direct oral anticoagulants (DOACs) or warfarin and on aspirin (ASA) for nonvalvular atrial fibrillation and/or venous thromboembolism, it is unclear if bleeding outcomes differ.
Objectives: To assess bleeding rates for ASA with DOACs vs warfarin and one another.
Methods: Registry-based cohort study of patients followed by a 6-center quality improvement collaborative in Michigan using data from 2009 to 2022. The study included adults on ASA with warfarin or DOACs for atrial fibrillation and/or venous thromboembolism without a recent myocardial infarction or heart valve replacement.
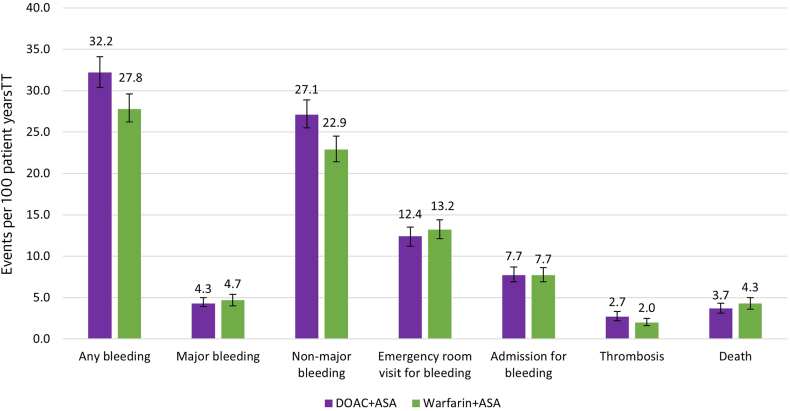
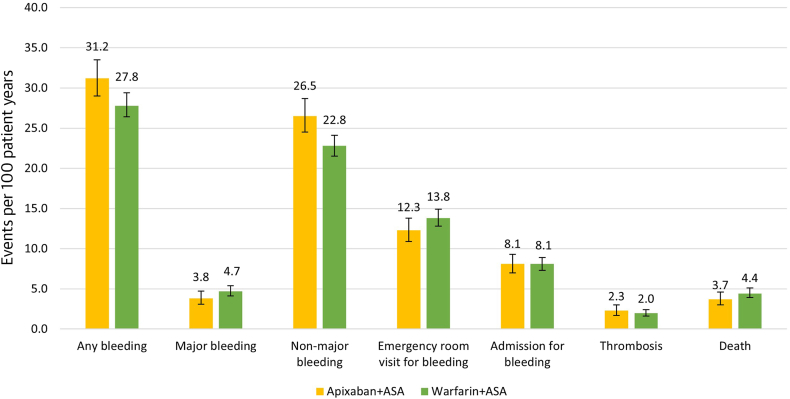
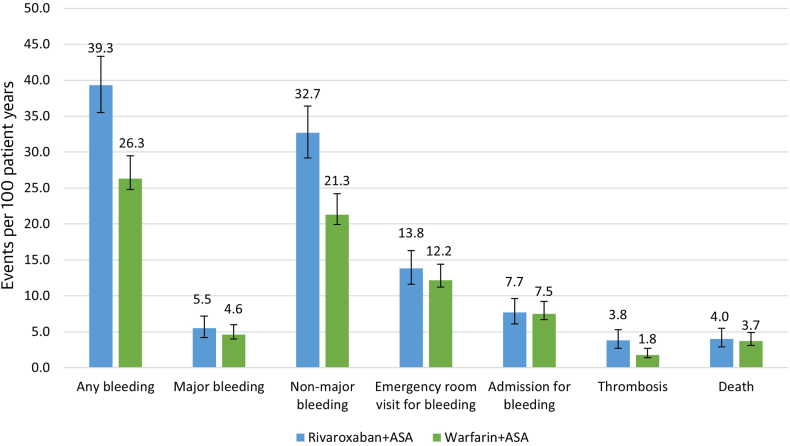
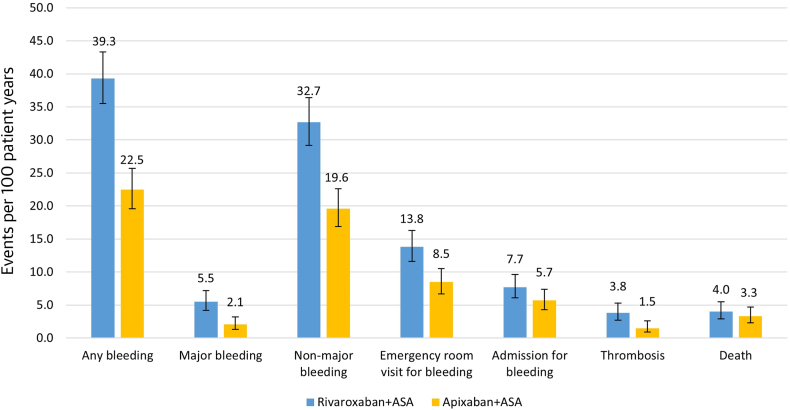
Results: After propensity matching by anticoagulant class, we compared 2 groups of 1467 patients followed for a median of 18.0 months. Any bleeding and nonmajor bleeding was increased with DOACs + ASA compared with warfarin + ASA (32.2 vs 27.8 and 27.1 vs 22.9 events/100 patient-years; relative risks [RRs], 1.1 and 1.2; 95% CIs, 1.1-1.2 and 1.1-1.3, respectively). After matching by drug, patients on apixaban + ASA vs warfarin + ASA had more bleeding (31.2 vs 27.8 events/100 patient-years; RR, 1.1; 95% CI, 1.0-1.2) and nonmajor bleeding but less major bleeding (3.8 vs 4.7 events/100 patient-years; RR, 0.8; 95% CI, 0.6-1.0) and emergency room visits for bleeding. Patients on rivaroxaban + ASA vs warfarin + ASA had more bleeding (39.3 vs 26.3 events/100 patient-years, RR, 1.5; 95% CI, 1.3-1.6), nonmajor bleeding, and thrombosis. Patients on apixaban + ASA vs rivaroxaban + ASA had significantly less bleeding (22.5 vs 39.3/100 patient-years; RR, 0.6; 95% CI, 0.5-0.7), nonmajor bleeding, major bleeding (2.1 vs 5.5 events/100 patient-years; RR, 0.4; 95% CI, 0.2-0.6), emergency room visits for bleeding, and thrombotic events.
Conclusion: Patients on DOAC + ASA without a recent myocardial infarction or heart valve replacement had more nonmajor bleeding but otherwise similar outcomes compared with warfarin + ASA. Patients treated with rivaroxaban + ASA experienced more adverse clinical events compared with warfarin + ASA or apixaban + ASA.
Keywords: aspirin; factor Xa inhibitors; hemorrhage; outcome assessment; warfarin.
© 2024 The Author(s).
Figures
Similar articles
-
Adverse Events Associated With the Addition of Aspirin to Direct Oral Anticoagulant Therapy Without a Clear Indication.JAMA Intern Med. 2021 Jun 1;181(6):817-824. doi: 10.1001/jamainternmed.2021.1197. JAMA Intern Med. 2021. PMID: 33871544 Free PMC article.
-
Comparison of real-world clinical and economic outcomes in patients receiving oral anticoagulants: A retrospective claims analysis.J Manag Care Spec Pharm. 2022 Nov;28(11):1304-1315. doi: 10.18553/jmcp.2022.28.11.1304. J Manag Care Spec Pharm. 2022. PMID: 36282935 Free PMC article.
-
Periprocedural Outcomes of Direct Oral Anticoagulants Versus Warfarin in Nonvalvular Atrial Fibrillation.Circulation. 2018 Oct 2;138(14):1402-1411. doi: 10.1161/CIRCULATIONAHA.117.031457. Circulation. 2018. PMID: 29794081
-
Association of Adding Aspirin to Warfarin Therapy Without an Apparent Indication With Bleeding and Other Adverse Events.JAMA Intern Med. 2019 Apr 1;179(4):533-541. doi: 10.1001/jamainternmed.2018.7816. JAMA Intern Med. 2019. PMID: 30830172 Free PMC article.
-
Direct Oral Anticoagulants vs. Vitamin K Antagonists in Atrial Fibrillation Patients at Risk of Falling: A Meta-Analysis.Front Cardiovasc Med. 2022 May 9;9:833329. doi: 10.3389/fcvm.2022.833329. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35615562 Free PMC article.
Cited by
-
Hemorrhage risk associated with triple antithrombotic therapy: a focused real-world pharmacovigilance disproportional analysis study.BMC Cardiovasc Disord. 2025 Mar 14;25(1):180. doi: 10.1186/s12872-025-04510-4. BMC Cardiovasc Disord. 2025. PMID: 40087557 Free PMC article.
-
Multidisciplinary Expert Guidance for the Management of Severe Bleeding on Oral Anticoagulation: An Algorithm for Practicing Clinicians.Thromb Haemost. 2025 Aug;125(8):717-732. doi: 10.1055/a-2464-2887. Epub 2024 Nov 8. Thromb Haemost. 2025. PMID: 39515380 Free PMC article. Review.
References
-
- Arnett D.K., Blumenthal R.S., Albert M.A., Buroker A.B., Goldberger Z.D., Hahn E.J., et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140:e596–e646. doi: 10.1161/CIR.0000000000000678. - DOI - PMC - PubMed
-
- US Preventive Services Task Force. Davidson K.W., Barry M.J., Mangione C.M., Cabana M., Chelmow D., et al. Aspirin use to prevent cardiovascular disease: US Preventive Services Task Force Recommendation Statement. JAMA. 2022;327:1577–1584. - PubMed
-
- Fihn S.D., Gardin J.M., Abrams J., Berra K., Blankenship J.C., Dallas A.P., et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: executive summary: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2012;126:3097–3137. - PubMed
-
- Fihn S.D., Blankenship J.C., Alexander K.P., Bittl J.A., Byrne J.G., Fletcher B.J., et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2014;64:1929–1949. - PubMed
-
- Gerhard-Herman M.D., Gornik H.L., Barrett C., Barshes N.R., Corriere M.A., Drachman D.E., et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2017;135:e686–e725. doi: 10.1161/CIR.0000000000000470. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
