

Mechanisms of action behind the protective effects of proactive esophageal cooling during radiofrequency catheter ablation in the left atrium
- PMID: 38984358
- PMCID: PMC11228283
- DOI: 10.1016/j.hroo.2024.05.002
Mechanisms of action behind the protective effects of proactive esophageal cooling during radiofrequency catheter ablation in the left atrium
Abstract
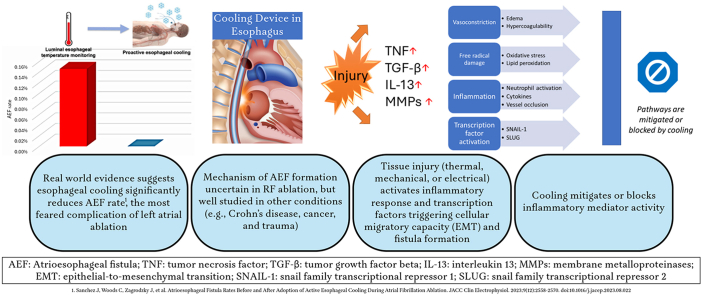
Proactive esophageal cooling for the purpose of reducing the likelihood of ablation-related esophageal injury resulting from radiofrequency (RF) cardiac ablation procedures is increasingly being used and has been Food and Drug Administration cleared as a protective strategy during left atrial RF ablation for the treatment of atrial fibrillation. In this review, we examine the evidence supporting the use of proactive esophageal cooling and the potential mechanisms of action that reduce the likelihood of atrioesophageal fistula (AEF) formation. Although the pathophysiology behind AEF formation after thermal injury from RF ablation is not well studied, a robust literature on fistula formation in other conditions (eg, Crohn disease, cancer, and trauma) exists and the relationship to AEF formation is investigated in this review. Likewise, we examine the abundant data in the surgical literature on burn and thermal injury progression as well as the acute and chronic mitigating effects of cooling. We discuss the relationship of these data and maladaptive healing mechanisms to the well-recognized postablation pathophysiological effects after RF ablation. Finally, we review additional important considerations such as patient selection, clinical workflow, and implementation strategies for proactive esophageal cooling.
Keywords: Atrial fibrillation; Atrioesophageal fistula; Esophageal cooling; Pulmonary vein isolation; Radiofrequency ablation.
© 2024 Heart Rhythm Society. Published by Elsevier Inc.
Figures

References
-
- Kapur S., Barbhaiya C., Deneke T., Michaud G.F. Esophageal injury and atrioesophageal fistula caused by ablation for atrial fibrillation. Circulation. 2017;136:1247–1255. - PubMed
-
- Della Rocca D.G., Magnocavallo M., Natale V.N., et al. Clinical presentation, diagnosis, and treatment of atrioesophageal fistula resulting from atrial fibrillation ablation. J Cardiovasc Electrophysiol. 2021;32:2441–2450. - PubMed
-
- Carroll B.J., Contreras-Valdes F.M., Heist E.K., et al. Multi-sensor esophageal temperature probe used during radiofrequency ablation for atrial fibrillation is associated with increased intraluminal temperature detection and increased risk of esophageal injury compared to single-sensor probe. J Cardiovasc Electrophysiol. 2013;24:958–964. - PubMed
-
- Muller P., Dietrich J.W., Halbfass P., et al. Higher incidence of esophageal lesions after ablation of atrial fibrillation related to the use of esophageal temperature probes. Heart Rhythm. 2015;12:1464–1469. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
