

Characterization and Mortality Risk of Impaired Left Ventricular Filling in Chronic Obstructive Pulmonary Disease
- PMID: 38984876
- PMCID: PMC12278002
- DOI: 10.1164/rccm.202310-1848OC
Characterization and Mortality Risk of Impaired Left Ventricular Filling in Chronic Obstructive Pulmonary Disease
Abstract
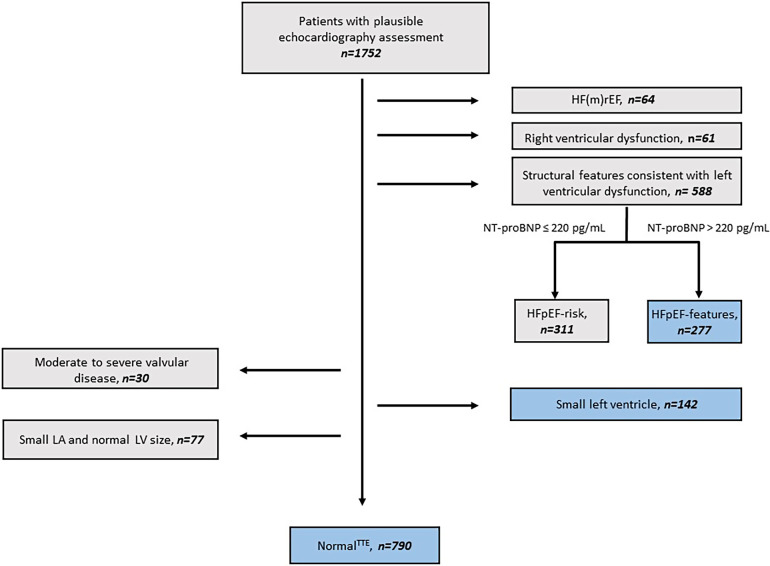
Rationale: In chronic obstructive pulmonary disease (COPD), impaired left ventricular (LV) filling might be associated with coexisting heart failure with preserved ejection fraction (HFpEF) or due to reduced pulmonary venous return indicated by small LV size. Objectives: We investigated the all-cause mortality associated with small LV or HFpEF and clinical features discriminating between both patterns of impaired LV filling in patients with COPD. Methods: We performed transthoracic echocardiography (TTE) in patients with stable COPD from the COSYCONET (COPD and Systemic Consequences and Comorbidities Network) cohort to define small LV as LV end-diastolic diameter below the normal range and HFpEF features according to recommendations of the European Society of Cardiology. We assessed the ratio of early to late ventricular filling velocity (E/A), ratio of early mitral inflow velocity to annular early diastolic velocity (E/e'), serum N-terminal pro-brain natriuretic peptide, high-sensitivity troponin I, airflow limitation (FEV1), lung hyperinflation (residual volume), and gas transfer capacity (DlCO) and discriminated patients with small LV from those with HFpEF features or no relevant cardiac dysfunction as per TTE (normalTTE). The primary outcome was all-cause mortality after 4.5 years. Measurements and Main Results: In 1,752 patients with COPD, the frequency of small LV, HFpEF features, and normalTTE was 8%, 16%, and 45%, respectively. Patients with small LV or HFpEF features had higher all-cause mortality rates than patients with normalTTE: hazard ratio, 2.75 (95% confidence interval, 1.54-4.89) and 2.16 (95% confidence interval, 1.30-3.61), respectively. Small LV remained an independent predictor of all-cause mortality after adjusting for confounders including exacerbation frequency and measures of residual lung volume, DlCO, or FEV1. Compared with normalTTE, patients with small LV had reduced LV filling, as indicated by lowered E/A. Yet, in contrast to patients with HFpEF features, patients with small LV had normal LV filling pressure (E/e') and lower concentrations of N-terminal pro-brain natriuretic peptide and high-sensitivity troponin I. Conclusions: In COPD, both small LV and HFpEF features are associated with increased all-cause mortality and represent two distinct patterns of impaired LV filling. Clinical trial registered with www.clinicaltrials.gov (NCT01245933).
Keywords: COPD; emphysema; heart failure with preserved ejection fraction; lung hyperinflation; ventricular underfilling.
Figures


Comment in
-
Echocardiographic Endophenotypes of Chronic Obstructive Pulmonary Disease: A Step toward Personalized Medicine.Am J Respir Crit Care Med. 2025 Mar;211(3):426-427. doi: 10.1164/rccm.202412-2461ED. Am J Respir Crit Care Med. 2025. PMID: 39879550 Free PMC article. No abstract available.
References
-
- Divo M, Cote C, de Torres JP, Casanova C, Marin JM, Pinto-Plata V, et al. BODE Collaborative Group Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med . 2012;186:155–161. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
