

Targeted Treatment Reverses Increased Left Cardiac Work in Unilateral vs. Bilateral Primary Aldosteronism
- PMID: 38985455
- PMCID: PMC11471835
- DOI: 10.1093/ajh/hpae087
Targeted Treatment Reverses Increased Left Cardiac Work in Unilateral vs. Bilateral Primary Aldosteronism
Abstract
Background: The incidence of cardiovascular complications may be higher in unilateral than bilateral primary aldosteronism (PA). We compared noninvasive hemodynamics after targeted therapy of bilateral vs. unilateral PA.
Methods: Adrenal vein sampling was performed, and hemodynamics recorded using radial artery pulse wave analysis and whole-body impedance cardiography (n = 114). In 40 patients (adrenalectomy n = 20, spironolactone-based treatment n = 20), hemodynamic recordings were performed after 33 months of PA treatment.
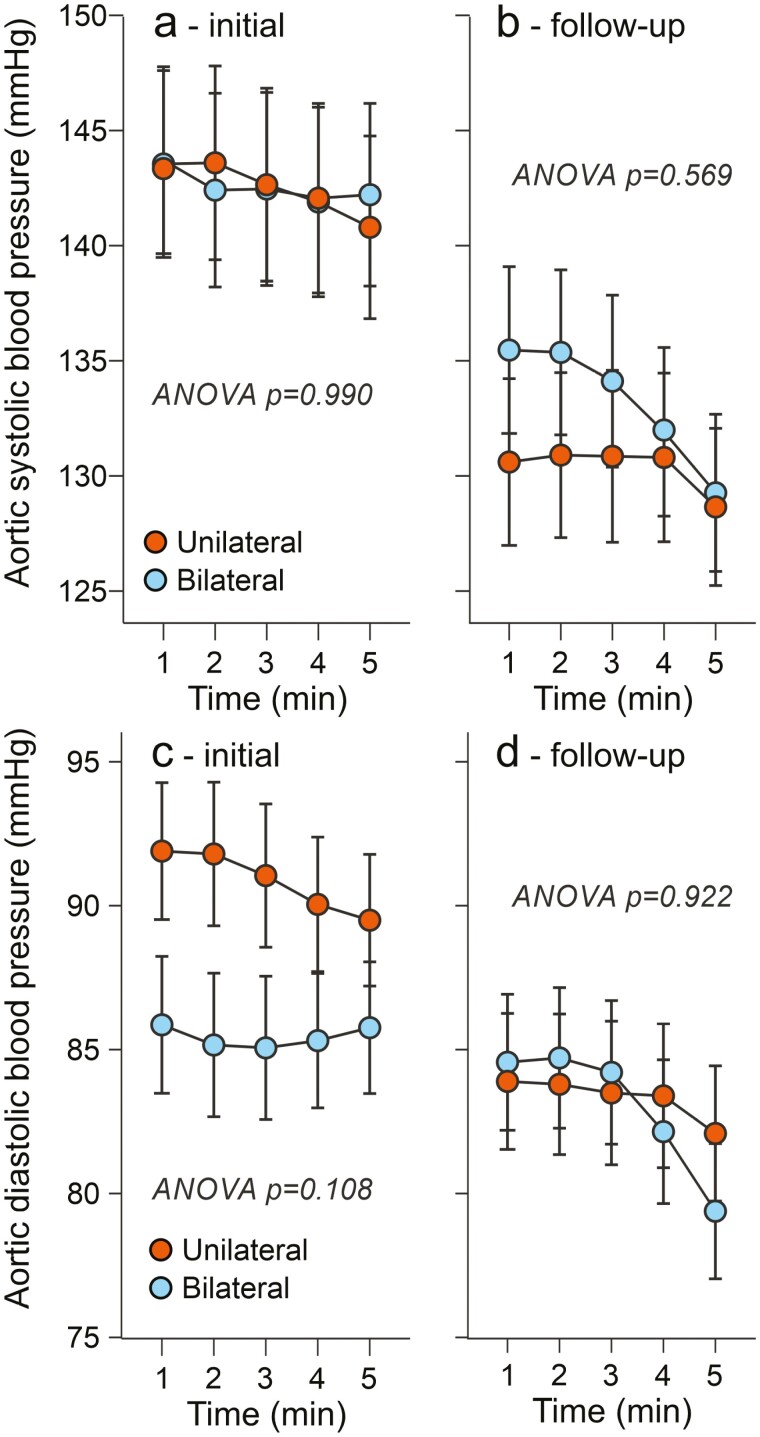
Results: In initial cross-sectional analysis, 51 patients had bilateral and 63 unilateral PA. The mean ages were 50.6 and 54.3 years (P = 0.081), and body mass indexes 30.3 and 30.6 kg/m2 (P = 0.724), respectively. Aortic blood pressure (BP) and cardiac output did not differ between the groups, but left cardiac work was ~10% higher in unilateral PA (P = 0.022). In the follow-up study, initial and final BPs in the aorta were not significantly different, while initial cardiac output (+13%, P = 0.015) and left cardiac work (+17%, P = 0.009) were higher in unilateral than bilateral PA. After median treatment of 33 months, the differences in cardiac load were abolished, and extracellular water volume was reduced by 1.3 and 1.4 l in bilateral vs. unilateral PA, respectively (P = 0.814).
Conclusions: These results suggest that unilateral PA burdens the heart more than bilateral PA, providing a possible explanation for the higher incidence of cardiac complications in unilateral disease. A similar reduction in aldosterone-induced volume excess was obtained with targeted surgical and medical treatment of PA.
Keywords: blood pressure; cardiac work; hypertension; primary aldosteronism.
© The Author(s) 2024. Published by Oxford University Press on behalf of American Journal of Hypertension, Ltd.
Conflict of interest statement
The authors declared no conflict of interest.
Figures




References
-
- Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, Stowasser M, Young WF.. The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2016; 101:1889–1916. - PubMed
-
- Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C, Ganzaroli C, Giacchetti G, Letizia C, Maccario M, Mallamaci F, Mannelli M, Mattarello MJ, Moretti A, Palumbo G, Parenti G, Porteri E, Semplicini A, Rizzoni D, Rossi E, Boscaro M, Pessina AC, Mantero F; PAPY Study Investigators. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol 2006; 48:2293–2300. - PubMed
-
- Monticone S, Burrello J, Tizzani D, Bertello C, Viola A, Buffolo F, Gabetti L, Mengozzi G, Williams TA, Rabbia F, Veglio F, Mulatero P.. Prevalence and clinical manifestations of primary aldosteronism encountered in primary care practice. J Am Coll Cardiol 2017; 69:1811–1820. - PubMed
-
- Heinrich DA, Adolf C, Rump LC, Quack I, Quinkler M, Hahner S, Januszewicz A, Seufert J, Willenberg HS, Nirschl N, Sturm L, Beuschlein F, Reincke M.. Primary aldosteronism: key characteristics at diagnosis: a trend toward milder forms. Eur J Endocrinol 2018; 178:605–611. - PubMed
-
- Reincke M, Bancos I, Mulatero P, Scholl UI, Stowasser M, Williams TA.. Diagnosis and treatment of primary aldosteronism. Lancet Diabetes Endocrinol 2021; 9:876–892. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 9AC076/State Funding for University-Level Health Research, Tampere University Hospital, Wellbeing Services County of Pirkanmaa
- SAT162/Finnish Foundation for Cardiovascular Research
- SAT124/Sigrid Jusélius Foundation
- MS885/Pirkanmaa Regional Fund of the Finnish Cultural Foundation
- Finnish Kidney Foundation
LinkOut - more resources
Full Text Sources
