

Prehospital Partial Resuscitative Endovascular Balloon Occlusion of the Aorta for Exsanguinating Subdiaphragmatic Hemorrhage
- PMID: 38985496
- PMCID: PMC11238066
- DOI: 10.1001/jamasurg.2024.2254
Prehospital Partial Resuscitative Endovascular Balloon Occlusion of the Aorta for Exsanguinating Subdiaphragmatic Hemorrhage
Abstract
Importance: Hemorrhage is the most common cause of preventable death after injury. Most deaths occur early, in the prehospital phase of care.
Objective: To establish whether prehospital zone 1 (supraceliac) partial resuscitative endovascular balloon occlusion of the aorta (Z1 P-REBOA) can be achieved in the resuscitation of adult trauma patients at risk of cardiac arrest and death due to exsanguination.
Design, setting, and participants: This was a prospective observational cohort study (Idea, Development, Exploration, Assessment and Long-term follow-up [IDEAL] 2A design) with recruitment from June 2020 to March 2022 and follow-up until discharge from hospital, death, or 90 days evaluating a physician-led and physician-delivered, urban prehospital trauma service in the Greater London area. Trauma patients aged 16 years and older with suspected exsanguinating subdiaphragmatic hemorrhage, recent or imminent hypovolemic traumatic cardiac arrest (TCA) were included. Those with unsurvivable injuries or who were pregnant were excluded. Of 2960 individuals attended by the service during the study period, 16 were included in the study.
Exposures: ZI REBOA or P-REBOA.
Main outcomes and measures: The main outcome was the proportion of patients in whom Z1 REBOA and Z1 P-REBOA were achieved. Clinical end points included systolic blood pressure (SBP) response to Z1 REBOA, mortality rate (1 hour, 3 hours, 24 hours, or 30 days postinjury), and survival to hospital discharge.
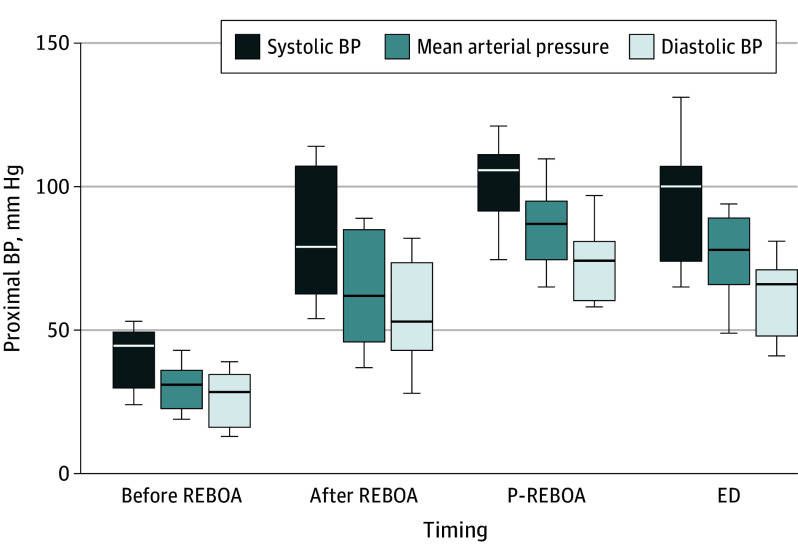
Results: Femoral arterial access for Z1 REBOA was attempted in 16 patients (median [range] age, 30 [17-76] years; 14 [81%] male; median [IQR] Injury Severity Score, 50 [39-57]). In 2 patients with successful arterial access, REBOA was not attempted due to improvement in clinical condition. In the other 14 patients (8 [57%] of whom were in traumatic cardiac arrest [TCA]), 11 successfully underwent cannulation and had aortic balloons inflated in Z1. The 3 individuals in whom cannulation was unsuccessful were in TCA (failure rate = 3/14 [21%]). Median (IQR) pre-REBOA SBP in the 11 individuals for whom cannulation was successful (5 [46%] in TCA) was 47 (33-52) mm Hg. Z1 REBOA plus P-REBOA was associated with a significant improvement in BP (median [IQR] SBP at emergency department arrival, 101 [77-107] mm Hg; 0 of 10 patients were in TCA at arrival). The median group-level improvement in SBP from the pre-REBOA value was 52 (95% CI, 42-77) mm Hg (P < .004). P-REBOA was feasible in 8 individuals (8/11 [73%]) and occurred spontaneously in 4 of these. The 1- and 3-hour postinjury mortality rate was 9% (1/11), 24-hour mortality was 27% (3/11), and 30-day mortality was 82% (9/11). Survival to hospital discharge was 18% (2/11). Both survivors underwent early Z1 P-REBOA.
Conclusions and relevance: In this study, prehospital Z1 P-REBOA is feasible and may enable early survival, but with a significant incidence of late death.
Trial registration: ClinicalTrials.gov Identifier: NCT04145271.
Conflict of interest statement
Figures

Comment in
-
Bringing REBOA Closer to the Point of Injury.JAMA Surg. 2024 Sep 1;159(9):1008. doi: 10.1001/jamasurg.2024.2233. JAMA Surg. 2024. PMID: 38985489 No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
