

The impact of discharge letter content on unplanned hospital readmissions within 30 and 90 days in older adults with chronic illness - a mixed methods study
- PMID: 38987669
- PMCID: PMC11238400
- DOI: 10.1186/s12877-024-05172-1
The impact of discharge letter content on unplanned hospital readmissions within 30 and 90 days in older adults with chronic illness - a mixed methods study
Abstract
Background: Care transitions are high-risk processes, especially for people with complex or chronic illness. Discharge letters are an opportunity to provide written information to improve patients' self-management after discharge. The aim of this study is to determine the impact of discharge letter content on unplanned hospital readmissions and self-rated quality of care transitions among patients 60 years of age or older with chronic illness.
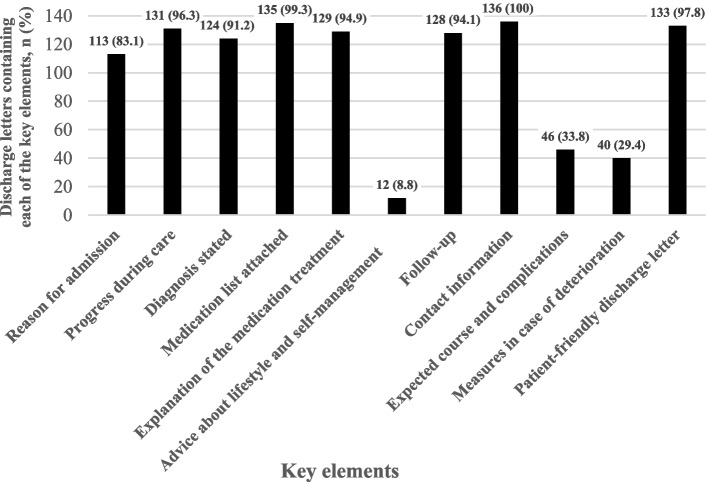
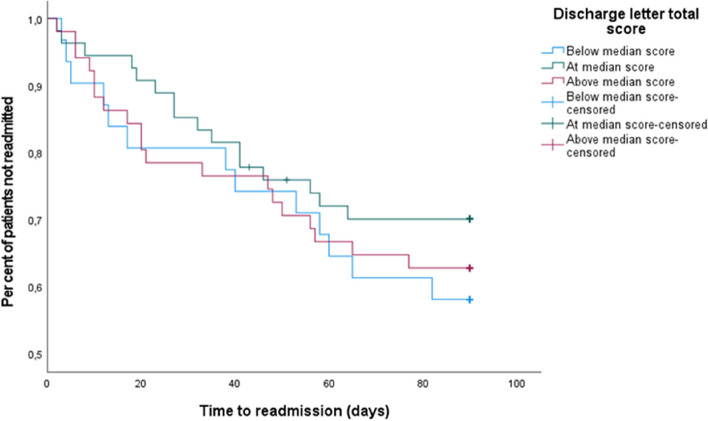
Methods: The study had a convergent mixed methods design. Patients with chronic obstructive pulmonary disease or congestive heart failure were recruited from two hospitals in Region Stockholm if they were living at home and Swedish-speaking. Patients with dementia or cognitive impairment, or a "do not resuscitate" statement in their medical record were excluded. Discharge letters from 136 patients recruited to a randomised controlled trial were coded using an assessment matrix and deductive content analysis. The assessment matrix was based on a literature review performed to identify key elements in discharge letters that facilitate a safe care transition to home. The coded key elements were transformed into a quantitative variable of "SAFE-D score". Bivariate correlations between SAFE-D score and quality of care transition as well as unplanned readmissions within 30 and 90 days were calculated. Lastly, a multivariable Cox proportional hazards model was used to investigate associations between SAFE-D score and time to readmission.
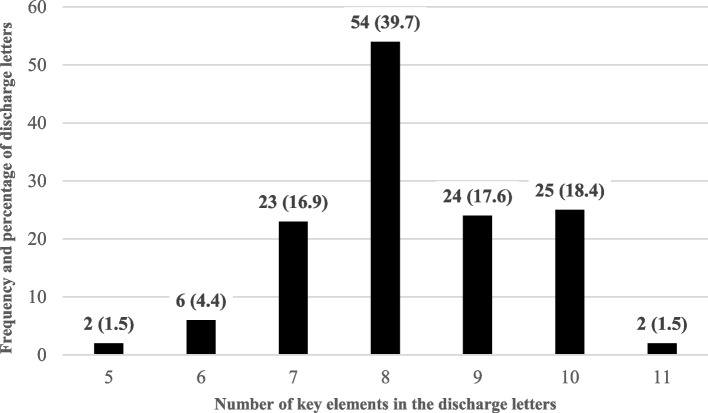
Results: All discharge letters contained at least five of eleven key elements. In less than two per cent of the discharge letters, all eleven key elements were present. Neither SAFE-D score, nor single key elements correlated with 30-day or 90-day readmission rate. SAFE-D score was not associated with time to readmission when adjusted for a range of patient characteristics and self-rated quality of care transitions.
Conclusions: While written summaries play a role, they may not be sufficient on their own to ensure safe care transitions and effective self-care management post-discharge.
Trial registration: Clinical Trials. giv, NCT02823795, 01/09/2016.
Keywords: Chronic obstructive pulmonary disease; Communication; Congestive heart failure; Hospital discharge; Medication therapy management; Polypharmacy; Self-management.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Heeren P, Devriendt E, Fieuws S, Wellens NIH, Deschodt M, Flamaing J, Sabbe M, Milisen K. Unplanned readmission prevention by a geriatric emergency network for transitional care (URGENT): a prospective before-after study. BMC Geriatr. 2019;19(1):215. doi: 10.1186/s12877-019-1233-9. - DOI - PMC - PubMed
-
- Provencher V, D'Amours M, Menear M, Obradovic N, Veillette N, Sirois MJ, Kergoat MJ. Understanding the positive outcomes of discharge planning interventions for older adults hospitalized following a fall: a realist synthesis. BMC Geriatr. 2021;21(1):84. doi: 10.1186/s12877-020-01980-3. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
