

Artificial intelligence-based screening for cardiomyopathy in an obstetric population: A pilot study
- PMID: 38989045
- PMCID: PMC11232425
- DOI: 10.1016/j.cvdhj.2024.03.005
Artificial intelligence-based screening for cardiomyopathy in an obstetric population: A pilot study
Abstract
Background: Cardiomyopathy is a leading cause of pregnancy-related mortality and the number one cause of death in the late postpartum period. Delay in diagnosis is associated with severe adverse outcomes.
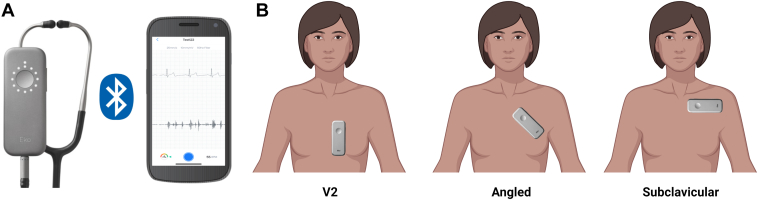
Objective: To evaluate the performance of an artificial intelligence-enhanced electrocardiogram (AI-ECG) and AI-enabled digital stethoscope to detect left ventricular systolic dysfunction in an obstetric population.
Methods: We conducted a single-arm prospective study of pregnant and postpartum women enrolled at 3 sites between October 28, 2021, and October 27, 2022. Study participants completed a standard 12-lead ECG, digital stethoscope ECG and phonocardiogram recordings, and a transthoracic echocardiogram within 24 hours. Diagnostic performance was evaluated using the area under the curve (AUC).
Results: One hundred women were included in the final analysis. The median age was 31 years (Q1: 27, Q3: 34). Thirty-eight percent identified as non-Hispanic White, 32% as non-Hispanic Black, and 21% as Hispanic. Five percent and 6% had left ventricular ejection fraction (LVEF) <45% and <50%, respectively. The AI-ECG model had near-perfect classification performance (AUC: 1.0, 100% sensitivity; 99%-100% specificity) for detection of cardiomyopathy at both LVEF categories. The AI-enabled digital stethoscope had an AUC of 0.98 (95% CI: 0.95, 1.00) and 0.97 (95% CI: 0.93, 1.00), for detection of LVEF <45% and <50%, respectively, with 100% sensitivity and 90% specificity.
Conclusion: We demonstrate an AI-ECG and AI-enabled digital stethoscope were effective for detecting cardiac dysfunction in an obstetric population. Larger studies, including an evaluation of the impact of screening on clinical outcomes, are essential next steps.
Keywords: Cardiomyopathies; ECG; Heart failure; Obstetrics; Postpartum; Pregnancy.
© 2024 Heart Rhythm Society.
Figures




References
-
- Regitz-Zagrosek V., Roos-Hesselink J.W., Bauersachs J., et al. 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy: the Task Force for the Management of Cardiovascular Diseases during Pregnancy of the European Society of Cardiology (ESC) Eur Heart J. 2018;39:3165–3241. - PubMed
-
- Germain S., Nelson-Piercy C. Common symptoms during pregnancy. Obstetrics, Gynaecology & Reproductive Medicine. 2011;21:323–326.
-
- ACOG ACOG Practice Bulletin No. 212: pregnancy and heart disease. Obstet Gynecol. 2019;133:e320–e356. - PubMed
LinkOut - more resources
Full Text Sources
