

Macrophage Migration Inhibitory Factor Promotes Thromboinflammation and Predicts Fast Progression of Aortic Stenosis
- PMID: 38989580
- PMCID: PMC11335082
- DOI: 10.1161/ATVBAHA.124.321000
Macrophage Migration Inhibitory Factor Promotes Thromboinflammation and Predicts Fast Progression of Aortic Stenosis
Abstract
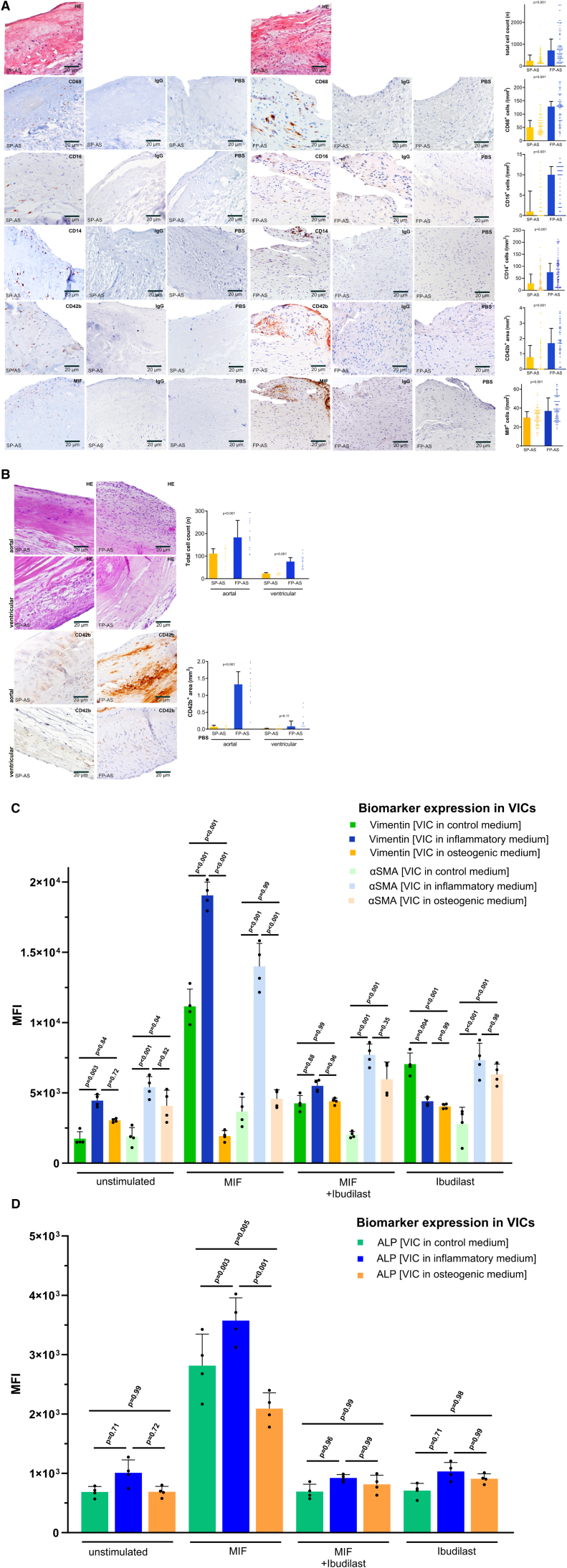
Background: Aortic stenosis (AS) is driven by progressive inflammatory and fibrocalcific processes regulated by circulating inflammatory and valve resident endothelial and interstitial cells. The impact of platelets, platelet-derived mediators, and platelet-monocyte interactions on the acceleration of local valvular inflammation and mineralization is presently unknown.
Methods: We prospectively enrolled 475 consecutive patients with severe symptomatic AS undergoing aortic valve replacement. Clinical workup included repetitive echocardiography, analysis of platelets, monocytes, chemokine profiling, aortic valve tissue samples for immunohistochemistry, and gene expression analysis.
Results: The patients were classified as fast-progressive AS by the median ∆Vmax of 0.45 m/s per year determined by echocardiography. Immunohistological aortic valve analysis revealed enhanced cellularity in fast-progressive AS (slow- versus fast-progressive AS; median [interquartile range], 247 [142.3-504] versus 717.5 [360.5-1234]; P<0.001) with less calcification (calcification area, mm2: 33.74 [27.82-41.86] versus 20.54 [13.52-33.41]; P<0.001). MIF (macrophage migration inhibitory factor)-associated gene expression was significantly enhanced in fast-progressive AS accompanied by significantly elevated MIF plasma levels (mean±SEM; 6877±379.1 versus 9959±749.1; P<0.001), increased platelet activation, and decreased intracellular MIF expression indicating enhanced MIF release upon platelet activation (CD62P, %: median [interquartile range], 16.8 [11.58-23.8] versus 20.55 [12.48-32.28], P=0.005; MIF, %: 4.85 [1.48-9.75] versus 2.3 [0.78-5.9], P<0.001). Regression analysis confirmed that MIF-associated biomarkers are strongly associated with an accelerated course of AS.
Conclusions: Our findings suggest a key role for platelet-derived MIF and its interplay with circulating and valve resident monocytes/macrophages in local and systemic thromboinflammation during accelerated AS. MIF-based biomarkers predict an accelerated course of AS and represent a novel pharmacological target to attenuate progression of AS.
Keywords: aortic valve stenosis; biomarkers; blood platelets; chemokines; inflammation.
Conflict of interest statement
None.
Figures





References
-
- Pawade TA, Newby DE, Dweck MR. Calcification in aortic stenosis: the skeleton key. J Am Coll Cardiol. 2015;66:561–577. doi: 10.1016/j.jacc.2015.05.066 - PubMed
-
- Chan KL, Teo K, Dumesnil JG, Ni A, Tam J; ASTRONOMER Investigators. Effect of lipid lowering with rosuvastatin on progression of aortic stenosis: results of the aortic stenosis progression observation: measuring effects of rosuvastatin (astronomer) trial. Circulation. 2010;121:306–314. doi: 10.1161/CIRCULATIONAHA.109.900027 - PubMed
-
- Yilmaz MB, Guray U, Guray Y, Cihan G, Caldir V, Cay S, Kisacik HL, Korkmaz S. Lipid profile of patients with aortic stenosis might be predictive of rate of progression. Am Heart J. 2004;147:915–918. doi: 10.1016/j.ahj.2003.11.011 - PubMed
-
- Mateos N, Gomez M, Homar A, Garcia-Elias A, Yáñez L, Tajes M, Molina L, Ble M, Cladellas M, Roqueta C, et al. . Plasmatic pcsk9 levels are associated with very fast progression of asymptomatic degenerative aortic stenosis. J Cardiovasc Transl Res. 2022;15:5–14. doi: 10.1007/s12265-021-10138-4 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
