

Applications of artificial intelligence in computed tomography imaging for phenotyping pulmonary hypertension
- PMID: 38989815
- PMCID: PMC11309337
- DOI: 10.1097/MCP.0000000000001103
Applications of artificial intelligence in computed tomography imaging for phenotyping pulmonary hypertension
Abstract
Purpose of review: Pulmonary hypertension is a heterogeneous condition with significant morbidity and mortality. Computer tomography (CT) plays a central role in determining the phenotype of pulmonary hypertension, informing treatment strategies. Many artificial intelligence tools have been developed in this modality for the assessment of pulmonary hypertension. This article reviews the latest CT artificial intelligence applications in pulmonary hypertension and related diseases.
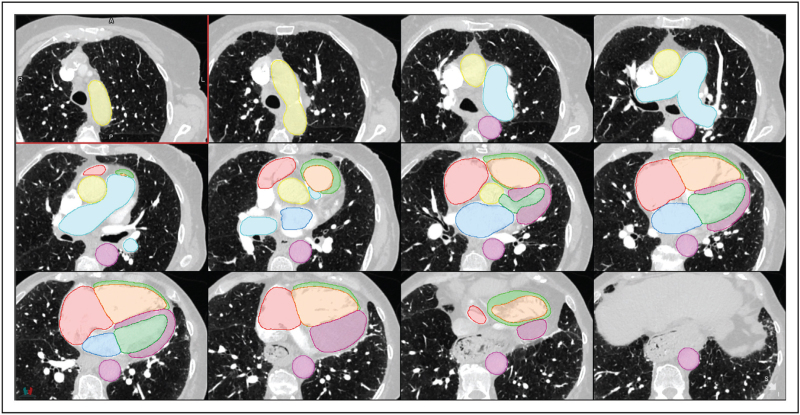
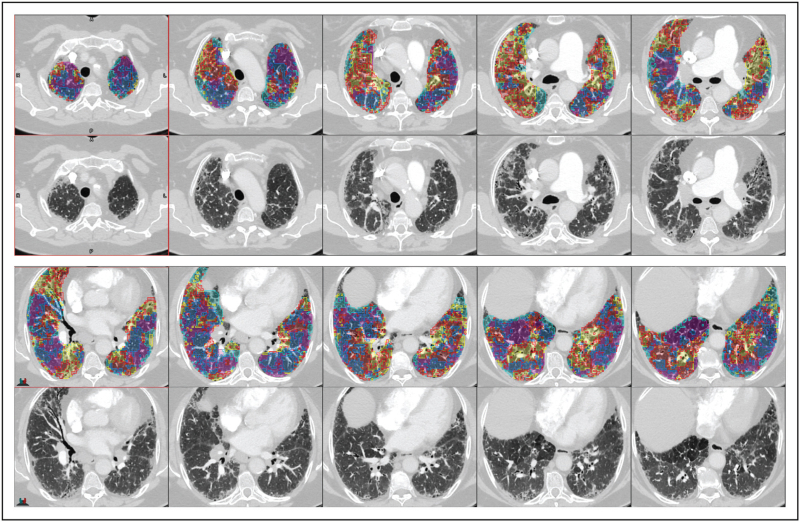
Recent findings: Multistructure segmentation tools have been developed in both pulmonary hypertension and nonpulmonary hypertension cohorts using state-of-the-art UNet architecture. These segmentations correspond well with those of trained radiologists, giving clinically valuable metrics in significantly less time. Artificial intelligence lung parenchymal assessment accurately identifies and quantifies lung disease patterns by integrating multiple radiomic techniques such as texture analysis and classification. This gives valuable information on disease burden and prognosis. There are many accurate artificial intelligence tools to detect acute pulmonary embolism. Detection of chronic pulmonary embolism proves more challenging with further research required.
Summary: There are numerous artificial intelligence tools being developed to identify and quantify many clinically relevant parameters in both pulmonary hypertension and related disease cohorts. These potentially provide accurate and efficient clinical information, impacting clinical decision-making.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Figures
Similar articles
-
External validation, radiological evaluation, and development of deep learning automatic lung segmentation in contrast-enhanced chest CT.Eur Radiol. 2024 Apr;34(4):2727-2737. doi: 10.1007/s00330-023-10235-9. Epub 2023 Sep 29. Eur Radiol. 2024. PMID: 37775589 Free PMC article.
-
Detection and quantification of pulmonary embolism with artificial intelligence: The SFR 2022 artificial intelligence data challenge.Diagn Interv Imaging. 2023 Oct;104(10):485-489. doi: 10.1016/j.diii.2023.05.007. Epub 2023 Jun 14. Diagn Interv Imaging. 2023. PMID: 37321875
-
Pulmonary Hypertension in Association with Lung Disease: Quantitative CT and Artificial Intelligence to the Rescue? State-of-the-Art Review.Diagnostics (Basel). 2021 Apr 9;11(4):679. doi: 10.3390/diagnostics11040679. Diagnostics (Basel). 2021. PMID: 33918838 Free PMC article. Review.
-
An artificial intelligence algorithm for pulmonary embolism detection on polychromatic computed tomography: performance on virtual monochromatic images.Eur Radiol. 2024 Jan;34(1):384-390. doi: 10.1007/s00330-023-10048-w. Epub 2023 Aug 5. Eur Radiol. 2024. PMID: 37542651
-
CT evaluation of chronic thromboembolic pulmonary hypertension.Clin Radiol. 2012 Mar;67(3):277-85. doi: 10.1016/j.crad.2011.09.012. Epub 2011 Nov 25. Clin Radiol. 2012. PMID: 22119298 Review.
Cited by
-
Experimental animal models and patient-derived platforms to bridge preclinical discovery and translational therapeutics in pulmonary arterial hypertension.J Transl Med. 2025 Jun 17;23(1):665. doi: 10.1186/s12967-025-06709-7. J Transl Med. 2025. PMID: 40528193 Free PMC article. Review.
-
PVRI International Conference 2025: Embracing Heterogeneity.Pulm Circ. 2025 May 1;15(2):e70093. doi: 10.1002/pul2.70093. eCollection 2025 Apr. Pulm Circ. 2025. PMID: 40321896 Free PMC article. No abstract available.
-
The Role of Computed Tomography and Artificial Intelligence in Evaluating the Comorbidities of Chronic Obstructive Pulmonary Disease: A One-Stop CT Scanning for Lung Cancer Screening.Int J Chron Obstruct Pulmon Dis. 2025 May 6;20:1395-1406. doi: 10.2147/COPD.S508775. eCollection 2025. Int J Chron Obstruct Pulmon Dis. 2025. PMID: 40352362 Free PMC article. Review.
-
Advancements in Machine Learning and Artificial Intelligence in the Radiological Detection of Pulmonary Embolism.Cureus. 2025 Jan 29;17(1):e78217. doi: 10.7759/cureus.78217. eCollection 2025 Jan. Cureus. 2025. PMID: 40026993 Free PMC article. Review.
References
-
- Humbert M, Kovacs G, Hoeper MM, et al. . 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J 2022; 43:3618–3731. - PubMed
-
Updated European guidelines for the diagnosis and management of pulmonary hypertension.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
